Risks Compared
Gardasil (HPV)
Worst case scenario of HPV: HPV can lead to cancerous and precancerous changes in the cervix.
Source: http://www.umm.edu/ency/article/000886.htm
Uncontested Serious Adverse Risks of the vaccine according to the product insert and the vaccine manufacturer: Erythema, Pelvic Inflammatory Disease, Asthma, Sepsis, Pancreatic Cancer, Arrhythmia (one of a few on here that can most certainly be fatal), Juvenile Arthritis, Rheumatoid Arthritis.
Source: http://www.merck.com/product/usa/pi_circulars/g/gardasil/gardasil_pi.pdf
Varivax (Varicella/Chickenpox)
Worse case scenario of Chickenpox: itchy, fluid filled blisters.
Source: http://www.umm.edu/ency/article/001592.htm
Uncontested Serious Adverse Risks of the vaccine according to the product insert and the vaccine manufacturer: Upper respiratory illness, arthralgia, allergic reactions, Anaphylaxis (including anaphylactic shock), angioneurotic edema, facial edema, peripheral edema, thrombocytopenia (including ITP), encephalitis, cerebrovascular accident, transverse myelitis, Guillain Barre Syndrome, Bell's Palsy, ataxia, non-febrile seizures, aseptic meningitis, paresthesia, pneumonia, pharyngitis, erythema multiforme, Henoch-schonlein purpura, secondary bacterial infections of skin and soft tissue, including impetigo and cellulitis, and herpes zoster.
Source: www.merck.com/product/usa/pi_circulars/v/varivax/varivaxpi.pdf
Rotarix (Rotavirus)
Worst case scenario of Rotavirus: Diarrhea leading to dehydration (treatable with re-hydration).
Source: http://www.umm.edu/ency/article/000252.htm
Uncontested Serious Adverse Risks of the vaccine according to the product insert and the vaccine manufacturer: Death and Kawasaki disease.
Source: http://www.fda.gov/CbER/label/rotarixLB.pdf
FluZone/FluShield (Influenza)
Worst case scenario of influenza: death from complications (rare in children, but possible).
Source: http://www.umm.edu/ency/article/000080.htm
Uncontested Serious Adverse Risks of the vaccine according to the product insert and the vaccine manufacturer: Anaphylaxis, Vasculitis, Neurological disorders such as Encephalopathy, optic neuritis/neuropathy, partial facial paralysis, brachial plexus, and neuropathy.
Source: www.fda.gov/CBER/label/fluzoneLB.pdf
The contestations with the influenza vaccine lie primarily in it's ingredients (it contains thimerosal), in the likelihood of a child experiencing influenza that may actually be life threatening versus the well known neurological impairments the vaccine does cause, and the total lack of efficiency of the vaccination.
More references on these topics:
***First of all, only about 20% of all flu-like illnesses are actually caused by an influenza virus, so it is important to keep in mind when you decide to give your child the flu vaccine that they are only getting a shot to protect them of a 20% out of 100% chance of flu illness, not the whole shebang.
-Source: FDA meeting, February 20th, 2003, as conceded by Nancy Cox, PhD, Chief Influenza Branch, Centers for Disease Control (CDC)
***The vaccine fails to get the proper flu strain contained on a regular basis, which means a serious risk for your child at a very unlikely benefit.
There are three main types of flu virus, and each type can mutate, or change, from year to year. Thus, there are literally thousands of possible strains. (Each strain is thoroughly analyzed and given a proper name, often a title associated with the place where it was initially discovered.) Every year health officials produce a new flu vaccine containing three mutated strains of flu virus. To determine which strains to use, officials travel to China at the beginning of the year to assess circulating flu viruses in that region of the world. They try to guess which strains will reach the United States by the end of the year. Production begins, and the new vaccine is usually available by October.
Flu "experts" often guess wrong. For example, in 1994 they predicted that Shangdong, Texas, and Panama strains would be prevalent that year, thus millions of people were vaccinated with a flu shot that contained these viruses. However, when winter arrived, the Johannesburg and Beijing strains of influenza circulated through society. The vaccine was ineffective. This happened again in 1996, and again in 1997. More recently, the vaccine created for the 2003-2004 flu season contained flu strains that did not circulate through society that year. Officials were once again forced to admit that millions of people were vaccinated with an ineffective vaccine. Yet, flu fatalities did not increase during these years. For example, in 1996, 857 people died from the flu; in 1997, 745 people died from the flu -- typical annual numbers.
In 2004, flu vaccine manufacturers were unable to produce enough flu shots to accommodate everyone who wanted a flu vaccine. (Several batches were contaminated and had to be destroyed.) Thus, only half of the population that is normally vaccinated against influenza (approximately 45 million people versus 90 million during an average year) received the vaccine. If influenza is truly a deadly disease, as officials claim, the 2004-2005 flu season should be catastrophic. If, as the CDC claims, 36,000 people die every year from the flu when 90 million people are vaccinated against the disease, how many more will die when only 45 million people are "protected?" I predict that flu fatalities will not increase. In fact, flu (and pneumonia?) fatalities may even decrease during this rare period when the American population is "under-vaccinated" against influenza.
Note: The article above was written in early 2005. On December 10, 2005, the British Medical Journal published a report acknowledging the veracity of this article by substantiating the claim that CDC flu death figures are completely bogus, hyper-inflated to scare the public and sell more flu vaccine.
-Additional source: British Medical Journal, "Are US flu death figures more PR than science?" http://thinktwice.com/BMJ_Flu.pdf
Primary Source: http://www.thinktwice.com/flu_lie.htm
There is also a vital inquiry to be made regarding whether the flu vaccine even prevents influenza deaths. In 2004, there was a massive shortage of flu vaccines due to a large number of contaminated batches. Supply was cut in half which should have resulted in a massive increase in influenza deaths in the United States. Yet instead of an increase in influenza deaths, there was a marked DECREASE- of 30%, in influenza deaths that year.
Sources:
CDC: "Deaths: final data for 2003". US Department of Health and Human Services; National Vital Statistics Reports (April 19, 2006); Volume 54, Number 13
CDC: "Deaths: final data for 2004". US Department of Health and Human Services; National Vital Statistics Reports (June 28, 2006); Volume 54, Number 19
MMRII (Measles Mumps Rubella): focus on measles in terms of risks but all would apply because they are contained within the same vaccination.
Worst case scenario of Measles: measles encephalitis: Inflammation of the brain (encephalitis), starting (up to 3 weeks) after onset of the rash and presenting with high fever, convulsions, and coma. It usually runs a short course with full recovery within a week. However it also may eventuate in central nervous system impairment or death.
Source: http://www.medterms.com/script/main/art.asp?articlekey=6370
Worst case scenario of Mumps: Orchitis: Inflammation of the testis (male sex organ). This may very rarely lead to sterility in a male.
Source:http://www.medterms.com/script/main/art.asp?articlekey=4660
Worst case scenario of Rubella: Rubella is most serious because of its ability to produce defects in a developing fetus if the mother is infected during early pregnancy. Congenital rubella syndrome occurs in 25% or more of infants born to women who acquired rubella during the first trimester of pregnancy. Defects are rare if the infection occurs after the 20th week of pregnancy. One or more defects may occur in an infected fetus and include deafness , cataracts , microcephaly , mental retardation , congenital heart defects , and other problems. A miscarriage or stillbirth may occur.
Source: http://www.umm.edu/ency/article/001574.htm
(Rubella is only a serious threat to pregnant women and their unborn children essentially. So why do we vaccinate little girls AND boys with this when we know vaccinations do not confer anywhere near lifelong or even long term immunity to disease?)
Uncontested Serious Adverse Risks of the vaccine according to the product insert and the vaccine manufacturer: 0- they officially admit nothing
"Possible" Serious Adverse Risks that the vaccine may cause but that they do not agree with a definitive association to: Panniculitis, Atypical measles, Vasculitis, Pancreatitis, Diabetes Mellitus, Thrombocytopenia, Leukocytosis, Anaphylaxis, Angioneurotic edema, Arthritis, Arthraliga, Polyneuritis, Encephalopathy or Encephalitis, Measles Inclusion Body Encephalitis (MIBE), Subacute Sclerosing Panencephalitis (SSPE), Convulsions or seizures, Ataxia, Polyneuropathy, Ocular palsies, Pneumonia, Erythema Multiforme, Urticaria, Otitis Media, Optic Neuritis, Papillitis, Retrobulbar neuritis, Epididymitis, Orchitis.
(that's a heck of a lot of "maybe's") TO CLARIFY WHAT IS MOST DEFINITELY CAUSED BY THE MMR VACCINE: ENCEPHALITIS!! WHICH IS THE ONLY SERIOUS THREAT OF MEASLES ITSELF AND ALSO SUBACUTE SCLEROSING PANENCEPHALITIS, WHICH UNLIKE TYPICAL MEASLES ENCEPHALITIS IS ALWAYS FATAL.
See the following references for more details:
Cavlek TV, Sternak SL, Subacute sclerosing panencephalitis--the continuing threat.
Coll Antropol. 2006 Dec;30(4):959-63
-------------------------------------
articles.mercola.com/sites/articles/archive/2008/01/02/mmr-vaccine-part-three.aspx
Measles-Mumps-Rubella (MMR) Vaccine as a Potential Cause of Encephalitis (Brain Inflammation) in Children
Harold E. Buttram, MD
The Physician's Desk Reference, in its section on the MMR vaccine, states that complications from MMR, such as encephalitis and optic neuritis, occur "very rarely."
--------------------------------------------------
www.bchealthguide.org/healthfiles/hfile14a.stm#E46E4
http://www.journals.uchicago.edu/doi/pdf/10.1086/520449
"Measles Inclusion Body Encephalitis Caused by the Vaccine Strain of Measles Virus"- PDF article on the topic
http://www.wpro.who.int/media_centre/fact_sheets/fs_20050606.htm
World Health Organization background information on Measles Vaccination
Measles vaccine safety
*May cause encephalitis
BC HealthFile #14a, September 2007
Measles, Mumps, Rubella (MMR) Vaccine
More serious reactions can include seizures caused by fever, a temporary drop in the blood cells that help prevent bleeding, and, inflammation of the brain (encephalitis).
------------------------------------------
IPOL (Poliomyelitis)
Worst case scenario of Polio: This infection can lead to temporary paralysis or, in more severe cases, permanent paralysis or death.
Source: http://www.umm.edu/ency/article/001402.htm
Uncontested Serious Adverse Risks of the vaccine according to the product insert and the vaccine manufacturer: 0- they officially admit nothing
"Possible" Serious Adverse Risks that the vaccine may cause but that they do not agree with a definitive association to: Guillain Barre Syndrome
Source: http://www.vaccineshoppe.com/US_PDF/IPOL_942420_11.06.pdf
THIS VACCINE UNDOUBTEDLY CAUSES PARALYTIC POLIO ITSELF! IN FACT THERE IS A MEDICAL TERM FOR IT EVEN- "PROVOCATION POLIO".
See the below references for details:
Sutter, Roland W., et al. "Attributable risk of DTP (Diphtheria and Tetanus Toxoids and Pertussis Vaccine) injection in provoking paralytic poliomyelitis during a large outbreak in Oman." Journal of Infectious Diseases 1992; 165:444-9.
Strebel, Peter M., et al. "Intramuscular injections within 30 days of immunization with oral poliovirus vaccine -- a risk factor for vaccine-associated paralytic poliomyelitis." New England J of Med (February 23, 1995), pp. 500+.
Editorial. "Provocation paralysis." Lancet 1992; 340:1005.
Wyatt, H.V. "Provocation poliomyelitis: neglected clinical observations from 1914-1950." Bulletin of Historical Medicine 1981; 55:543-57.
Guyer, B., et al. "Injections and paralytic poliomyelitis in tropical Africa." Bull WHO 1980; 58:285-91.
Wyatt, H.V. "Incubation of poliomyelitis as calculated from time of entry into the central nervous system via the peripheral nerve pathways." Rev Infect Dis 1990; 12:547-56.
Wyatt H.V., et al. "Unnecessary injections and paralytic poliomyelitis in India." Trans R Soc Trop Med Hyg 1992; 86:546-49.
***Polio vaccine has also been responsible for the carcinogen SV-40. Unfortunately some bad monkey kidney cells happened to invade many batches of Polio vaccines (since monkey kidney cells are one of the ingredients in the polio vaccine) and this has caused a massive, and very hidden, incidence of Cancer in the United States because of the nature of this contamination. Below is documentation regarding the connection.
http://thinktwice.com/s_polio.htm
1. Monkey kidneys are used to develop polio vaccines.
2. SV-40, a cancer-causing virus, thrived in monkey kidneys.
3. Polio vaccines were contaminated.
4. Millions of people in the USA and throughout the world were infected.
5. Cancer rates have increased. SV-40 is found in brain tumors, bone cancers, lung cancers, and leukemia.
Sources:
Shah, K and Nathanson, N. "Human exposure to SV40." American Journal of Epidemiology, 1976; 103: 1-12.
Innis, M.D. "Oncogenesis and poliomyelitis vaccine." Nature, 1968; 219:972-73.
Soriano, F., et al. "Simian virus 40 in a human cancer." Nature, 1974; 249:421-24.
Weiss, A.F., et a;. "Simian virus 40-related antigens in three human meningiomas with defined chromosome loss." Proceedings of the National Academy of Science 1975; 72(2):609-13.
Scherneck, S., et al. "Isolation of a SV-40-like papovavirus from a human glioblastoma." International Journal of Cancer 1979; 24:523-31.
Stoian, M., et al. "Possible relation between viruses and oromaxillofacial tumors. II. Research on the presence of SV40 antigen and specific antibodies in patients with oromaxillofacial tumors." Virologie, 1987; 38:35-40.
Stoian, M., et al. "Possible relation between viruses and oromaxillofacial tumors. II. Detection of SV40 antigen and of anti-SV40 antibodies in patients with parotid gland tumors." Virologie, 1987; 38:41-46
. Bravo, M.P., et al. "Association between the occurrence of antibodies to simian vacuolating virus 40 and bladder cancer in male smokers." Neoplasma, 1988; 35:285-88.
O'Connell, K., et al. "Endothelial cells transformed by SV40 T-antigen cause Kaposi?s sarcoma-like tumors in nude mice." American Journal of Pathology, 1991; 139(4):743-49.
Weiner, L.P., et al. "Isolation of virus related to SV40 from patients with progressive multifocal leukoencephalopathy." New England Journal of Medicine, 1972; 286:385-90.
Tabuchi, K. "Screening of human brain tumors for SV-40-related T-antigen." International Journal of Cancer 1978; 21:12-17.
Meinke, W., et al. "Simian virus 40-related DNA sequences in a human brain tumor." Neurology 1979; 29:1590-94.
Krieg, P., et al. "Episomal Simian Virus 40 Genomes in Human Brain Tumors." Proceedings of the National Academy of Sciences of the USA, 1981, 78(10):6446-6450.
Krieg, P., et al. "Cloning of SV40 genomes from human brain tumors." Virology 1984; 138:336-40.
Geissler, E. "SV40 in human intracranial tumors: passenger virus or oncogenic 'hit-and-run' agent?" Z Klin Med, 1986; 41:493-95.
Geissler, E. "SV40 and Human Brain Tumors." Progress in Medical Virology, 1990; 37:211-222.
Bergsagel, D.J., et al. "DNA sequences similar to those of simian virus 40 in ependymomas and choroid plexus tumors of childhood." New England Journal of Medicine, 1992; 326:988-93.
Martini, M., et al. "Human Brain Tumors and Simian Virus 40." Journal of the National Cancer Institute, 1995, 87(17):1331.
Lednicky, JA., et al. "Natural Simian Virus 40 Strains are Present in Human Choroid Plexus and Ependymoma Tumors." Virology, 1995, 212(2):710-17.
Tognon, M., et al. "Large T Antigen Coding Sequence of Two DNA Tumor Viruses, BK and SV-40, and Nonrandom Chromosome Changes in Two Gioblastoma Cell Lines." Cancer Genetics and Cytogenics, 1996, 90(1): 17-23.
Carbone, M., et al. "SV-40 Like Sequences in Human Bone Tumors." Oncogene, 1996, 13(3):527-35.
Pass, HI, Carbone, M., et al. "Evidence For and Implications of SV-40 Like Sequences in Human Mesotheliomas." Important Advances in Oncology, 1996, pp. 89-108.
Rock, Andrea. "The Lethal Dangers of the Billion Dollar Vaccine Business," Money, (December 1996), p. 161. [Article]
Carlsen, William. "Rogue virus in the vaccine: Early polio vaccine harbored virus now feared to cause cancer in humans." San Francisco Chronicle (July 15, 2001), p. 7. [Article: Research by Susan Fisher, epidemiologist, Loyola University Medical Center.]
Bookchin, D. and Schumacher J. "Tainted polio vaccine still carries its threat 40 years later." The Boston Globe (January 26, 1997). [Article]
Rosa, FW., et al. "Absence of antibody response to simian virus 40 after inoculation with killed-poliovirus vaccine of mothers offspring with neurological tumors." New England Journal of Medicine, 1988; 318:1469.
Rosa, FW., et al. Response to: "Neurological tumors in offspring after inoculation of mothers with killed poliovirus vaccine." New England Journal of Medicine, 1988, 319:1226.
Martini, F., et al. "SV-40 Early Region and Large T Antigen in Human Brain Tumors, Peripheral Blood Cells, and Sperm Fluids from Healthy Individuals." Cancer Research, 1996, 56(20):4820-4825.
(We'll say it once and a thousand times after that: animal junk byproducts do not belong in human bodies! Let alone with the total lack of proper inspection and safety that goes into creating these vaccines!)
Infanrix DTaP (Diphtheria Tetanus and Pertussis/Whooping Cough)
Worst case scenario of Diphtheria: inflammation of the heart muscle; temporary paralysis.
Source: http://www.umm.edu/ency/article/001608.htm
Worst case scenario of Tetanus: death.
Source: http://www.umm.edu/ency/article/000615.htm
Worst case scenario of Pertussis: death.
Source: http://www.umm.edu/ency/article/001561.htm
Uncontested Serious Adverse Risks of the vaccine according to the product insert and the vaccine manufacturer: Brachial neuritis, Anaphylactic reaction, Guillain Barre Syndrome, Arthus-type local reactions.
"Possible" Serious Adverse Risks that the vaccine may cause but that they do not agree with a definitive association to: Intusussception, Idiopathic Thrombocytopenic Purpura, Thrombocytopenia, Encephalopathy, Hypotonic-hyporesponsive episodes (HHE's), SIDS, Cyanosis, Cellulitis, Convulsions, Erythema.
Concerns with Tetanus element: Tetanus itself does not confer (even temporary) immunity. So how is the vaccination, which is supposed to mimic a diseases' natural conference of immunity, supposed to be effective?
Sources:
National Center for Emergency Medicine Informatics- http://www.neemi.org/ese/ese1020.htm
Tetanus and Polio Vaccines- Some Facts for Parents who are Worried About These Diseases, Jan 1998; Viera Scheibner, PhD
Furthermore, the Tetanus portion of the vaccination is so diluted (due to the high toxicity of Tetanus) that it is effectively chemical laced tapwater.
Source:
Tetanus Toxoid Vaccination, an overview by Kris Gaublomme MD, available at http://www.whale.to/v/tetanus.html
Concerns with Pertussis element:
***The United States still sees outbreaks of Pertussis despite far-exceeding "herd immunity" standards of immunization rates for the disease, with the vast majority of the cases occurring in vaccinated children. Not only that, but the CDC itself admits that Pertussis cases are (and have been) on the rise for quite some time now. It's obvious the vaccination is pathetically ineffective at preventing the disease and the risks of the vaccine are severe.
CDC references/admittance:
"Since the early 1980’s, reported Pertussis cases have been increasing, with peaks every 3-4 years."
www.cdc.gov/vaccines/vac-gen/whatifstop.htm
(note that there are several more pertussis vaccination doses recommended now than there were in the 1980's and the vaccination rate is, contrary to media inference, actually higher now than it was then as well.)
"Over the past five to six years, the nation has seen a spike in pertussis, said Dr. Richard Tooker, chief medical …. The Centers for Disease Control and Prevention says the United States has about 5,000 to 7,000 reported cases each year. The incidence of the disease has been increasing steadily since the 1980s….the vaccine has not been effective as long as was planned, he said."
-Mah, Linda S, Mlive.com -- 2006- 9-22
Parents understand there is some risk to any medicine we give our children, but if we are going to take a risk, especially some of the more serious risks this vaccination carries, we have a right to know that we are not taking that risk as a gamble (for potentially no reason at all), and that the medicine we are giving them is going to work.
Havrix (Hepatitis A)
Worst case scenario of Hepatitis A: flu like symptoms.
Source: http://umm.edu/ency/article/000278.htm
Uncontested Serious Adverse Risks of the vaccine according to the product insert and the vaccine manufacturer: Pharyngitis, Dysgeuisa, Hypertonia, Photophobia, "Creatine phosphokinase increase".
Source: http://us.gsk.com/products/assets/us_havrix.pdf
For anyone not understanding what any of the risk diseases mean according to the product insert I'll give you an explanation of the worst one, hypertonia. Hypertonia can lead to loss of function, deformity, and cerebral palsy.
(http://www.medterms.com/script/main/art.asp?articlekey=3850)
Your doctor feels the risk of this condition is worth your child not getting flu like symptoms, and furthermore, when the risk of Hepatitis A is also virtually eliminated by proper handwashing. (www.909shot.com/Diseases/hepatitis%20a.html)
Energix B (Hepatitis B)
Worst case scenario of Hepatitis B: permanent liver damage, cirrhosis and liver cancer due to chronic infection.
Source: http://www.umm.edu/ency/article/000279.htm
Uncontested Serious Adverse Risks of the vaccine according to the product insert and the vaccine manufacturer: Hypotension, Arthralgia, Erythema Multiforme (Stevens-Johnson Syndrome), Anaphylaxis, Angioedema, Tachycardia, Arthritis, Dyspepsia, Transverse Myelitis, Hypoesthesia, Guillain Barre Syndrome, Bell's Palsy, Thrombocytopenia, Herpes Zoster.
Source: http://us.gsk.com/products/assets/us_engerixb.pdf
Concerns:
***It's a fact- the only chance your child has of contracting Hepatitis B is if you (the mother) pass it onto them in vitro, or if they are sharing intravenous needles and having un-protected sex with multiple partners (not a common behavior of infants and toddlers, assumedly). Routine blood screening of pregnant women is all that is needed to prevent the extremely rare instance of Hepatitis B in infants and children.
***There is a mighty long list of admitted and potentially life threatening adverse events associated with this immunization. It carries a substantially higher rate of serious adverse reaction than any other vaccine (although the HPV vaccine, Gardasil, is rapidly catching up) and has no basis for use in infants and toddlers without infected mothers whatsoever.
References on the high rate of risk of Hepatitis B vaccination:
Geier MR; "Hepatitis B vaccination safety." Ann Pharmacother 2002 Mar;36(3):370-4
Medical Literature Cites Immune System/Brain Damage - During the past decade, there have been many reports in the medical literature (primarily in international medical journals rather than U.S. medical journals) that hepatitis B vaccination is causing chronic immune and neurological disease in children and adults, including lupus:
Tudela & Bonal (1992); Mamoux & Dumont (1994); Guiserix (1996); arthritis, including polyarthritis and rheumatoid arthritis: Christan & Helin (1987); Hachulla et al (1990); Rogerson & Nye (1990); Biasi et al (1993),(1994); Vautier & Carty (1994); Hassan & Oldham (1994); Rheumatic Review (1994); Gross et al (1995); Pope et al (1995); Cathebras et al (1996); Soubrier et al (1997); Guillain Barre Syndrome GBS): Shaw et al (1988), Tuohy (1989); demyelinating disorders such as optic neuritis, Bell's Palsy, demyelinating neuropathy, transverse myelitis and multiple sclerosis: Shaw et al (1988); WHO (1990); Reutens et al (1990); Herroelen et al (1991); Nadler (1993); Brezin et al (1993); Mahassin et al (1993); Kaplanski et al (1995); Baglivo et al (1996); Marsaudon & Barrault (1996); Berkman et al (1996); Waisbren (1997); diabetes mellitus: Poutasi (1996); Classen (1996); chronic fatigue: Salit (1993); Delage et al (1993); vascular disorders: Fried et al (1987); Goolsby (1989); Cockwell et al (1990); Poullin & Gabriel (1994); Mathieu et al (1996); Graniel et al (1997); and others.
Hep B Vaccine Infant Deaths Reported In VAERS - Even though fewer than 10 percent of all doctors report health problems following vaccination, there are more than 16,000 reports of hospitalizations, injuries and deaths following hepatitis B vaccination that have been reported to the U.S. government Vaccine Adverse Event Reporting System (VAERS) since July 1990. There are reports of deaths in infants under one month of age following hepatitis B vaccination in VAERS, with most of the deaths being classified as sudden infant death syndrome (SIDS), even though SIDS is not historically recognized in the medical literature as occurring in babies under two months of age.
www.909shot.com/Diseases/hepbnlr.htm
***Hepatitis B vaccine has also been causally linked to Multiple Sclerosis. While the United States government and vaccine manufacturers refuse to admit an official association, France has, and is rewarding money in lawsuits from vaccine injured citizens claiming that their MS was caused by the Hepatitis B vaccine. Please read below for further documentation on Multiple Sclerosis and the recombinant Hepatitis B vaccine.
Sources:
Rouge-Maillart CI; "Recognition by French courts of compensation for post-vaccination multiple slcerosis: the consequences with regard to expert practice." Med Sci Law. 2007 Jul;47(3):185-90
Comenge Y; "Multiple sclerosis and hepatitis b vaccination: adding the credibility of molecular biology to an unusual level of clinical and epidemiological evidence." Med Hypotheses 2006;66(1):84-6
Fare E; "Multiple sclerosis and hepatitis B vaccination: could minute contamination of the vaccine by partial hepatitis b virus polymerase play a role through molecular mimicry?" Med Hypotheses, 2005;65(3)509-20
"These findings are consistent with the hypothesis that immunization with recombinant hepatitis B vaccine is associated with an increased risk of MS, and challenge the idea that the relation between hepatitis B vaccination and risk of MS is well understood."
-Hernan MA; "Recombinant hepatitis B vaccine and the risk of multiple sclerosis: a prospective study." Neurology 2004 Sep 14;63(5):838-42
Vial T; "Autoimmune diseases and vaccniations." Eur J Dermatol. 2004 Mar-Apr;14(2):86-90
There will be separate articles written regarding the meningitis vaccinations for Hib, Pneumococcal and Meningococcal, as these are all of a more complex nature than the vaccinations listed here and have lengthy risk profiles.
Thursday, October 29, 2009
Smallpox Eradication
Smallpox
*CDC Statistics: www.cdc.gov/Features/SmallpoxEradication
Their “Timeline” for smallpox eradication:
1796: The first smallpox vaccine was developed by Edward Jenner.
After WWI (which ended officially in 1919): Most of Europe Smallpox free.
After WWII (which ended officially in 1945): Transmission interrupted in Europe and North America.
1950: The Pan American Sanitary Organization, the predecessors to the Pan American Health Organization, undertook a program to eradicate smallpox in the Western Hemisphere.
1958: The first proposal for global eradication was made to the World Health Assembly by the USSR in 1958. They proposed a worldwide vaccination program to be completed in a 3 to 5 year period.
1966: The World Health Assembly decided to intensify the eradication program by providing a special budget of $2.4 million per year specifically for this effort.
1967: The Intensified Global Eradication program began: an estimated 10-15 million smallpox cases still occurred in 31 countries where the disease was endemic.
By the end of 1975, smallpox persisted only in the Horn of Africa.
An even more intensive surveillance containment and vaccination program was initiated in the spring and summer of 1977. As a result, the world’s last indigenous patient with smallpox on earth was a hospital cook in Merka, Somalia on October 26, 1977 with variola minor.
*The Rebuttal: there is much to be desired in terms of quality information in the CDC’s “Smallpox Eradication” page. Very little details were given, only a seemingly tossed together timeline with no specific information that was designed to leave the impression that Smallpox was a miracle vaccination that saved countless lives. Yet where does the true detail behind these timelines lie?
Let us examine their leap from 1796 to the end of WWI, which occurred in 1919: suddenly, after a development of the vaccine, Europe became “mostly” Smallpox free. Here is some more detailed information about what happened globally with the Smallpox vaccine and in the incidence of Smallpox disease in that timeframe:
Japan started compulsory vaccination against smallpox in 1872 and continued it for many years with disastrous results. Smallpox steadily increased each year and in 1892 their records showed 165,774 cases with 29,979 deaths -- all vaccinated. During the same time period Australia had no compulsory vaccination laws. The records showed only three deaths from smallpox over 15 years.
In the Philippines between 1917 and 1919, the U.S. government staged a compulsory vaccination campaign which brought on the worst epidemic of smallpox in this island nation's history with 162,503 reported cases and 71,453 deaths -- all vaccinated.
Dr. Charles Nichols of Boston gave this indictment:
“In India, according to an official return presented to the British House of Commons by Viscount Morley, there have been, during 30 years, 1877 to 1906, 3,344,325 deaths from smallpox of persons presumably vaccinated, for vaccination is universally enforced in India....In each and every community where vaccination ceases and strict sanitation is substituted, smallpox disappears. There are no exceptions to this.”
In Anne Riley Hale's 1935 book, The Medical VooDoo, she recounts the history of England's smallpox vaccination and resulting epidemics. The compulsory smallpox vaccination law was in effect when England experienced the disastrous smallpox epidemic of 1871-1873. This prompted the appointment of the Royal Commission in 1889 to thoroughly investigate the entire history of vaccination in the United Kingdom.
The Royal Commission sat for seven years gathering evidence which led to the repeal of England's compulsory vaccination law.
They received statistical analysis from eminent scientists and medical doctors which showed that the epidemics increased dramatically after 1854 -- the year the compulsory vaccination law went into effect. In the London epidemic of 1857-1859, there were 14,244 deaths; in the 1863-1865 outbreak - 20,059 deaths; and from 1871-1873 all of Europe was swept by the worst smallpox epidemic in recorded history.
In England and Wales alone, 44,840 people died of smallpox at a time when, according to official estimates, 97 percent of the population had been vaccinated.
They received statistical analysis from eminent scientists and medical doctors which showed that the epidemics increased dramatically after 1854 -- the year the compulsory vaccination law went into effect. In the London epidemic of 1857-1859, there were 14,244 deaths; in the 1863-1865 outbreak - 20,059 deaths; and from 1871-1873 all of Europe was swept by the worst smallpox epidemic in recorded history.
In England and Wales alone, 44,840 people died of smallpox at a time when, according to official estimates, 97 percent of the population had been vaccinated.
It was also noted how the smallpox vaccine contributed to the spread of syphilis. The Royal Commission admitted in its Sixth Report a list of 1,000 'vaccino-syphilis' cases submitted to them as evidence they could not deny of the association. Dr. Charles Creighton, professor of Microscopic Anatomy at Cambridge and author of Epidemics of Great Britain was commissioned by Encyclopedia Britannica to assemble information on syphilis (9th Ed, Vol 24, p 23), reported that “in the first year of compulsory vaccination (1854), deaths from syphilis among infants under one year of age suddenly increased by one half, and the increase has gone on steadily since.”
-Source: Smallpox: Setting the Record Straight By Vaccination Liberation, June 2008 Idaho Observer
In England, compulsory vaccination against smallpox was first introduced in 1852, yet in the period 1857 to 1859, a smallpox epidemic killed 14,244 people. In 1863 to 1865, a second epidemic claimed 20,059 lives. In 1867, a more stringent compulsory vaccination law was passed and those who evaded vaccination were prosecuted. After an intensive tour year effort to vaccinate the entire population between the ages of 2 - 50, the Chief Medical Officer of England announced in May 1871 that 97.5% had been vaccinated. In the following year, 1872, England experienced its worst ever smallpox epidemic which claimed 44,840 lives. Between 1871-1880, during the period of compulsory vaccination, the death rate from smallpox leapt from 28 to 46 per 100,000 population.
Writing in the British Medical Journal (21/1/1928 p116) Dr L Parry questions the vaccination statistics which revealed a higher death rate amongst the vaccinated than the unvaccinated and asks:
"How is it that smallpox is five times as likely to be fatal in the vaccinated as in the unvaccinated?
"How is it that in some of our best vaccinated towns - for example, Bombay and Calcutta - smallpox is rife, whilst in some of our worst vaccinated towns, such as Leicester, it is almost unknown?
"How is it that something like 80 per cent of the cases admitted Into the Metropolitan Asylums Board smallpox hospitals have been vaccinated, whilst only 20 per cent have not been vaccinated?
"How is it that in Germany, the best vaccinated country in the world, there are more deaths in proportion to the population than In England - for example, in 1919, 28 deaths in England, 707 In Germany; In 1920, 30 deaths In England, 354 In Germany In Germany In 1919 There were 5,012 cases of smallpox with 707 deaths; in England In 1925 There were 5,363 cases of smallpox with 6 deaths. What is the explanation?"
In Scotland, between 1855-1875, over 9,000 children under 5 died of smallpox despite Scotland being, at that time, one of the most vaccinated countries in the world. In 1907- 1919 with only a third of the children vaccinated, only 7 smallpox deaths were recorded for children under 5 years of age.
In Germany, in the years 1870-1 871, over 1,000,000 people had smallpox of which 120,000 died. 96% of these had been vaccinated. An address sent to the governments of the various German states from Bismarck, the Chancellor of Germany, contained the following comments:
"... the hopes placed in the efficacy of the cowpox virus as preventative of smallpox have proved entirely deceptive".
In an article, Vaccination In Italy' which appeared In the New York Medical Journal, July 1899, Chas Rauta, Professor of Hygiene and Material Medical in the University of Perguia, Italy, points out:
"Italy is one of the best vaccinated countries in the world, if not the best of all, for twenty years before 1885, our nation was vaccinated in the proportion of 98.5%. Notwithstanding, the epidemics of smallpox that we have had have been something so frightful that nothing before the invention of vaccination could equal them. During 1887, we had 16,249 deaths from smallpox; in 1888- 18,110 and 1889, 131413".
-Source: Smallpox by Ian Sinclair. http://www.whale.to/vaccines/sinclair.html
*ICAV’s notes: Now let us examine the “eradication” of Smallpox in developing nations that occurred from the late 1960’s forward. While the CDC states that such “eradication” was the result of mass immunization, many theorize that Smallpox was simply, and similarly to Polio, labeled differently in reporting standards, namely as “Monkeypox” or “Varicella” (chicken pox) in an attempt to hide the Smallpox vaccines ineffectiveness and to promote present and future mass immunization. The following references are available for review:
The manipulation of statistics to support England's compulsory smallpox vaccine is discussed in literature distributed by The National Anti-Vaccination League of Britain. For instance, “The Ministry of Health has admitted that the vaccinal condition is a guiding factor in diagnosis.”
This means that if a person who is vaccinated comes down with the disease he is “protected” against, the disease is simply recorded under another name. From 1904 to 1934 in England and Wales, 3,112 died of chicken pox and 579 died of smallpox according to the health records. In other words, people who have been vaccinated for smallpox and later come down with the disease are classified in the health records as having chickenpox, a non-fatal disease.
George Bernard Shaw said, “During the last considerable epidemic at the turn of the century, I was a member of the Health Committee of London Borough Council, and I learned how the credit of vaccination is kept up statistically by diagnosing all the revaccinated cases [of smallpox] as pustular eczema, varioloid or what not -- except smallpox.”
-Source: Smallpox: Setting the Record Straight By Vaccination Liberation, June 2008 Idaho Observer
There are many questions about the role of the vaccine in the decline of the disease, a point which may be clarified in a later issue of IVN. However, it is questionable whether smallpox really was eradicated as we have been told. Some publications stated that the last smallpox virus had disappeared from this globe. But had it really?
Certainly not, since viruses were stored and even used in later experiments as ‘carrier molecules’ for an experimental AIDS vaccine. Some of the volunteers engaged by the Pasteur Institute died during the experiment from a smallpox-like illness (1). The institute managed to keep the information out of the front pages.
A new and embarrassing development was the resurgence of pox-family viruses in Africa, known as the ‘monkeypox’. This fact has been known for many years but the public was reassured that this had nothing to do with smallpox and that the human species was safe.
Not as safe as we were told, though, since in the Congo in 1970, pox viruses were isolated from humans2 corresponding to the pox viruses found in captive monkeys in 1958 and identified the next year (3). It was baptised ‘monkeypox~. The same virus was isolated from 6 humans in 1959 by Foster. In 1976, Gipsen reported on more cases in Nigeria (4).
The terminology of the disease became ever more confusing, since what were at first simply ‘monkeypox’ are now introduced into literature as‘human monkeypox’. What, now, is the difference between smallpox and ‘human monkeypox’? It is interesting to read in a recent article in the Lancet that "Human monkeypox is a systemic exanthem, resembling smallpox, that occurs as a sporadic zoonosis in rural rainforest villages of western and central Africa. The disease is caused by an orthopoxvirus, which is transmitted to human beings by handling infected animals; serosurveys have implicated squirrels ... as the probable reservoir. Secondary human-to-human spread by aerosol or direct contact accounts for about 28% of cases..." (my emphasis)
So, let us make a simple addition. This virus is an ‘orthopox’ virus, which means, literally translated, a ‘real pox’ virus. This virus spreads among humans causing an exanthem ‘resembling’ smallpox, and causing disease and death among the infected (between February and August 1996, 71 cases were notified in the Katako-Kombe area in Zaire, 6 of which 4 died from the disease (5).
So what is the difference between smallpox and human monkeypox? The difference is a difference in protein structure. Nucleotide sequence analysis revealed different structures. But what does this really matter it both viruses affect us in the same way, spread in the same way, and cause the same eruptions and the same clinical disease? Scientists do, the victims don’t!
It is quite odd that the authors do not mention the smallpox vaccination status of the infected. All they mention is that in a ‘preliminary study’ none of the examined had a scar of smallpox vaccination. Which does not mean that they had not been vaccinated as the vaccine may not have ‘taken’. No figures are available about antibodies against smallpox, so that we have no real clue whether, in this study, the vaccine showed any protection against monkeypox or not. Many of the patients described elsewhere were vaccinated. Arita and Henderson (6) found 94 children with facial scarring caused by monkeypox; all except two who also showed scars typical for smallpox vaccination. So the least one can do is to question the protection offered by smallpox vaccination against the new monkey-pox virus.
Apparently the new virus is quite infectious, since 42 cases, including 3 deaths, were reported in a small village with only 346 inhabitants. The article further states that "present cluster of cases constitutes a reemergence of human monkeypox on a scale greater in magnitude than the approximate 65 annual cases previously indicated for Kasai Oriental, Bandundu, and Equateur regions from 1981 to 1986" and also that "it contains a more extensive occurrence of person-to-person transmission than previously recognised."
The conclusion of the authors is that" Because sequence analyses have indicated that Zairian monkeypox strains have not diverged greatly from the first isolate from the area in 1970 and monkeypox and smallpox variola viruses are independently evolved species (7), notions of monkeypox virus mutating into variola virus are unfounded." This does not sound very reassuring.
Former suggestions that "prolonged episodes or sustained cascades of transmission of human monkeypox would be unlikely" (8) do not hold up. Although the smallpox VIRUS appears to have died down a few decades ago, obviously the DISEASE is still present on this earth and able to make a come-back. Whether this is due to the mutation of the original virus or to a new virus that generates the same disease is a question that remains unanswered.
REFERENCES:
1. Personal communication with a staff member.
2. Mukinda, V.B.K.; et al Reemergence of human monkeypox in Zaire in 1996. Lancet, 1997; 349:1449-50
3. von Magnus, P.; et al A pox-like disease In cynomolgus monkeys. Acta Pathologica et Microbiologica Scandinavica, 1959; 46/2:156-76
4. Gipsen, R.; et al Monkeypoxspecific antibodies in human and simian sera from the ivory Coast and Nigeria. Bull, WHO, 1976; 53; 355-60 5. WHO. Monkeypox, Zaire. Widy Epidemiol Aec, 1996; 71:326
6. Arita, I.; Henderson, D.A.; Monkey-pox and whitepox viruses in West and Central Africa.Bull WHO, 1976; 53:347-53
7. Douglass, N.; Dumbell, K.R.; Independent evolution of monkeypox and variola viruses. J Virol, 1992; 66:7565-7
8. Jezek, Z.; Fenner, F.; Human monkeypox. Monographs In Virology Vol 17, J.L.Melnick, ed. Basel, Switzerland:Karger, 1988
-Source: Dr. Kris Gaublomme, Has smallpox really disappeared from the earth? The International Vaccination Newsletter, Dec 1997
“It is claimed by medical historians that the vaccination process wiped out smallpox throughout the world. However, the truth is that compulsory vaccination was abandoned because more deaths were caused by the vaccinations than there were cases of smallpox. A slight of the hand trick was used to foster the claim that smallpox was eradicated by the vaccination practice. Everyone who had been vaccinated and who developed smallpox was diagnosed as having chicken pox!”
-Source: Smallpox By Dr. Vivian Virginia Vetrano 11-2-2
*ICAV leaves you with the following thoughts on Smallpox vaccination:
“It is pertinent that James Phipps, the eight year old boy vaccinated by Jenner in l896, died at the age of 20. He had been re-vaccinated twenty times. Jenner's own son who had also been vaccinated died at the young age of twenty-one. Both succumbed to tuberculosis, a condition that some researchers have linked to the smallpox vaccine.”- Eleanor McBean, The Poisoned Needle
"One of the medical profession’s greatest boasts is that it eradicated smallpox through the use of the smallpox vaccine. I myself believed this claim for many years. But it simply isn’t true. One of the worst smallpox epidemics of all time took place in England between 1870 and 1872 – nearly two decades after compulsory vaccination was introduced. After this evidence that smallpox vaccination didn’t work the people of Leicester in the English midlands refused to have the vaccine any more. When the next smallpox epidemic struck in the early 1890s the people of Leicester relied upon good sanitation and a system of quarantine. There was only one death from smallpox in Leicester during that epidemic. In contrast the citizens of other towns (who had been vaccinated) died in vast numbers. ......Doctors and drug companies may not like it but the truth is that surveillance, quarantine and better living conditions got rid of smallpox – not the smallpox vaccine......It is worth pointing out that Edward Jenner, widely feted as the inventor of the smallpox vaccine, tried out the first smallpox vaccination on his own 10 month old son. His son remained mentally retarded until his death at the age of 21. Jenner refused to have his second child vaccinated. "---- Dr Vernon Coleman MB
"Smallpox was on the way out, indeed epidemics disappeared decades before the WHO decided to conduct the final "eradication" campaign. It is also well-documented that the largest epidemics occurred in the most highly vaccinated populations, while whose who were unvaccinated, did not have the same epidemics. "--.Viera Scheibner, PhD
"Vaccination for smallpox was fraudulently inaugurated and dishonestly maintained to the financial and health cost to the public which is beyond estimation. It did little or nothing to eradicate smallpox in endemic areas, has been directly responsible for thousands of deaths since its inception in the UK alone, and has sown the seeds of disease throughout the world."---Michael Nightingale
"My experience of small-pox during those six years of bedside attendance has given me the right, or rather has imposed on me the duty, of taking part in the bold and spirited onslaught on Vaccination, which is now being carried on in Switzerland, Germany, England, and other countries ... I am convinced that Vaccination is the greatest mistake and delusion in the science of medicine; a fanciful illusion in the mind of the discoverer; a phenomenal apparition devoid of scientific foundation, and wanting in all the conditions of scientific possibility."—Dr. JOSEPH HERMANN, Head Physician to the Imperial Hospital, Vienna, from 1858 to 1864: (Source: [1876] THE STATISTICS OF THE MEDICAL OFFICERS TO THE LEEDS SMALL-POX HOSPITAL EXPOSED AND REFUTED
"What, then, is the value of vaccination? We firmly believe that it has no value at all. Its supposed value has been deduced from incorrect reasoning on the part of its advocates. Were small-pox as prevalent and as fatal now as in the eighteenth century, it might even be justifiable to have recourse to inoculation—either by variolous or vaccine matter. History, however, has demonstrated that towards the close of the last century, when Jenner introduced his system, small-pox had gradually died out, as we shall presently show. Even in Jenner's day small-pox had lost its virulence."---Dr. Charles T. Pearce, M.D. [1868 Book: Essay on Vaccination]
"Whether we examine the long-continued records of London mortality, or those of modern registration for England, Scotland, and Ireland; whether we consider the "control experiment" or crucial test afforded by unvaccinated Leicester, or the still more rigid test in the other direction, of the absolutely revaccinated Army and Navy, the conclusion is in every case the same: that vaccination is a gigantic delusion; that it has never saved a single life; but that it has been the cause of so much disease, so many deaths, such a vast amount of utterly needless and altogether undeserved suffering, that it will be classed by the coming generation among the greatest errors of an ignorant and prejudiced age, and its penal enforcement the foulest blot on the generally beneficent course of legislation during our century."-----ALFRED RUSSEL WALLACE [Book 1898] VACCINATION A DELUSION
FURTHERMORE:
Smallpox vaccine -=fail AND 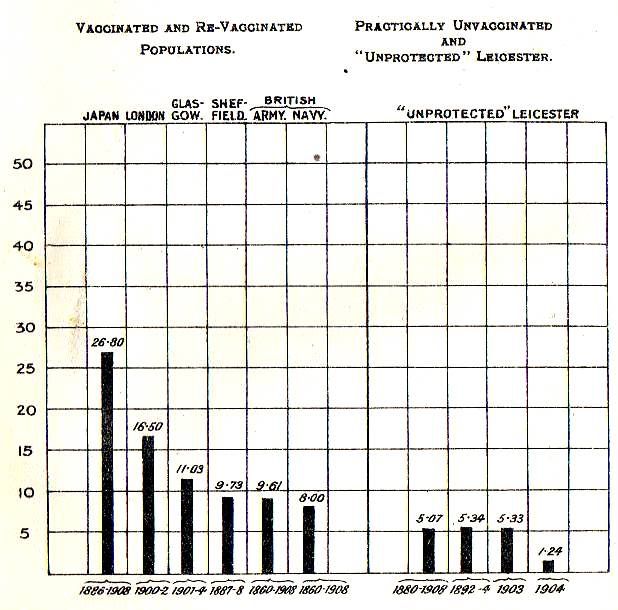
The above chart is the number of smallpox deaths in the fully vaccinated populations versus the unvaccinated ones.
the smallpox vaccine sure killed a lot of people too!!
New info:
------------------------------------------------------------------------------------------
From 1796 forward the smallpox vaccine has been implemented, universally enforced in Europe and the US from the early 1800's and used all over the world otherwise in manners exceeding herd immunity standards (yes including Africa and other undeveloped nations) and there were still 300-500 million cases of it... in the TWENTIETH century!
"Of all the poxviruses, smallpox in particular has played a gruesome role in human history. The virus is estimated to have caused between 300 million and 500 million deaths in the 20th century alone. Though smallpox was declared officially eradicated in 1979, many experts fear that clandestine samples of the virus may have survived -- thus making it a major bioterrorism concern."
Are Vaccinations Really Backed By Reliable Safety Testing and Clinical Trials?
Most parents (and physicians alike) assume that vaccinations undergo rigorous safety testing and clinical trials before they are released. The appropriate level of research conducted on vaccinations should be double blind placebo controlled studies with follow up monitoring for a few years... you would think. In the unfortunate and dismal reality of vaccine safety testing however, not only are most vaccines not tested against placebos (let alone with double blind studies) there may also be a pathetically miniscule number of trial participants, safety trials that leave out participants of the age group that is actually vaccinated, and a duration of monitoring post trial that would make even the most ethically flexible scientist cringe.
The details, followed by the product insert links so you can check for yourself if so inclined:
MMRII: the Measles, Mumps and Rubella Vaccination
The safety trial only observed 284 participants aged 11 months to 7 years. Merck did not even bother to state the duration of the trial or the duration or method of monitoring.
http://www.merck.com/product/usa/pi_circulars/m/mmr_ii/mmr_ii_pi.pdf
INFANRIX: the Diphtheria, Tetanus and Pertussis (DTaP) Vaccine
There were 407 infants monitored for only 8 days. The vaccination was not compared to a control, but to the whole cell DTP vaccine.
http://us.gsk.com/products/assets/us_infanrix.pdf
I-POL: the Polio Vaccine
The I-pol vaccine safety and clinical trials are a bit of an eyebrow raiser. While they do claim there were 1,300 infants (aged 2, 4 and 18 months) in the trial, they state that 4 different trials made up this group of infants. There is no information regarding location, method, duration of monitoring, etcetera. The I-pol vaccine was also not compared to a control such as saline but rather to the whole cell DTP vaccine. Interestingly the product insert states that the I-pols adverse reactions were "comparable in frequency and severity to that reported for DTP given alone." (the whole cell DTP vaccine which was banned because it was too dangerous to administer... that's reassuring!)
https://www.vaccineshoppe.com/US_PDF/IPOL_942420_11.06.pdf
Act-HiB: the Haeomophilus Influenzae Type B Vaccine
401 infants were observed in the safety trials, that's it. There was no duration of monitoring or methodological details listed. As an odd sidebar they did include the random factor that 3 of the 401 infants suffered seizures. (wonder why the CDC doesn't have THAT 'vaccine adverse reaction statistic' on their website)
http://www.novaccine.com/pdffiles/Act_HIB_package_insert.pdf
Havrix: the Hepatitis A Vaccine
According to the product insert, there were an enormous number of participants: 32,900, engaged in 60 clinical trials! Which is pretty... interesting. How exactly and why exactly did they choose to do it that way?? At any rate, the information posted for the two principle safety trials (the only ones they include any information about specifically on the p.i.): The first stated it was compared to the Energix B vaccination, the second stated it was compared to Infanrix DTaP vaccination and a conjugatae HiB vaccine (both). Duration of monitoring on the first study was not noted, however in the second study the amount of duration was only 4 days post vaccination via the use of "diary cards" given to the parents.
http://us.gsk.com/products/assets/us_havrix.pdf
Energix B: the Hepatitis B Vaccine
Every trial participant in this clinical and safety trial were 6 years or older! This vaccination is administered to infants 12 hours out of the womb and given regularly on the recommended childhood immunization schedule otherwise from birth through five! Talk about an obtuse methodological error. The vaccine was also compared not to a control but to another vaccination.
http://us.gsk.com/products/assets/us_engerixb.pdf
Prevnar: the Pneumococcal Vaccine
Was tested against another vaccine and not a control (an "investigative" aka experimental, Men C vaccine no less). No specific date of monitoring for adverse reactions was given but the product insert did state "the pre protocol analysis of the primary end point included cases which occured >14 days after the third dose."
http://www.wyeth.com/content/showlabeling.asp?id=134
Menactra: the Meningococcal Vaccine
The vaccination was compared to the Menomune vaccination and not a control. There were 7 days of solicited monitoring post vaccination via "diary cards" included in the 28 days of unsolicited adverse reaction monitoring post vaccination (aka if the parent had something happen to their child they could report it within those 28 days, but nobody would be contacting them after the intial 7 days to find out).
https://www.vaccineshoppe.com/image.cfm?doc_id=8826&image_type=product_pdf
Fluzone: the Influenza Vaccine
Was not compared to a control. Safety study included a total of 31 children (19 children aged 6 to 23 months and 12 children aged 24 to 36 months), that's it! They were given two total doses of vaccines spaced one month apart and local and systemic reactions were only solicited for 3 days post vaccination.
https://www.vaccineshoppe.com/image.cfm?doc_id=10913&image_type=product_pdf
Note: the Rotavirus and Gardasil vaccinations were the only ones that checked out for being placebo controlled and appropriately conducted. Good job guys!
Unfortunately these are two vaccinations designed for totally mild conditions which both admit to a causative association with FATALITY. If it wasn't such a terrible combination, you would think God had a keen sense of humor. The only two appropriately researched vaccinations are the ones made for innocuous conditions and they can cause death in their recipients? Woooow.
If you don't believe me check out the Rotavirus vaccine product insert which concedes to an uncontested causation of death (which is oddly the reason the first rotavirus vaccine got banned, although the manner of death was different... I guess it takes them a while to learn!):
http://www.fda.gov/BiologicsBloodVaccines/Vaccines/ApprovedProducts/ucm133920.htm
Or the Gardasil vaccine product insert which concedes to an uncontested causation of arrhythmia, which can most certainly be fatal, among a VERY long list of debilitating diseases including Asthma, Sepsis, Pancreatic cancer and rheumatoid arthritis.
http://www.merck.com/product/usa/pi_circulars/g/gardasil/gardasil_pi.pdf
The point of this article on safety studies is clear: the next time you get the thought that the FDA or any other governmental entity is absolutely ensuring your safety with it's "rigid" safety testing standards of drugs and pharmaceutical products, please think again! If this is how pathetic the standards are for testing chemicals that are going to be injected into infants bodies is, imagine how "stringent" the standards must be for adult medicines.
Always make sure you look at the product inserts for yourself before consenting to using any pharmaceutical product. There is a laundry list of FDA approved drugs out there that carry more serious adverse reaction risks than the condition they were designed to treat. And never forget, being a smart patient benefits you as well as your physician. Thanks for reading.
The details, followed by the product insert links so you can check for yourself if so inclined:
MMRII: the Measles, Mumps and Rubella Vaccination
The safety trial only observed 284 participants aged 11 months to 7 years. Merck did not even bother to state the duration of the trial or the duration or method of monitoring.
http://www.merck.com/product/usa/pi_circulars/m/mmr_ii/mmr_ii_pi.pdf
INFANRIX: the Diphtheria, Tetanus and Pertussis (DTaP) Vaccine
There were 407 infants monitored for only 8 days. The vaccination was not compared to a control, but to the whole cell DTP vaccine.
http://us.gsk.com/products/assets/us_infanrix.pdf
I-POL: the Polio Vaccine
The I-pol vaccine safety and clinical trials are a bit of an eyebrow raiser. While they do claim there were 1,300 infants (aged 2, 4 and 18 months) in the trial, they state that 4 different trials made up this group of infants. There is no information regarding location, method, duration of monitoring, etcetera. The I-pol vaccine was also not compared to a control such as saline but rather to the whole cell DTP vaccine. Interestingly the product insert states that the I-pols adverse reactions were "comparable in frequency and severity to that reported for DTP given alone." (the whole cell DTP vaccine which was banned because it was too dangerous to administer... that's reassuring!)
https://www.vaccineshoppe.com/US_PDF/IPOL_942420_11.06.pdf
Act-HiB: the Haeomophilus Influenzae Type B Vaccine
401 infants were observed in the safety trials, that's it. There was no duration of monitoring or methodological details listed. As an odd sidebar they did include the random factor that 3 of the 401 infants suffered seizures. (wonder why the CDC doesn't have THAT 'vaccine adverse reaction statistic' on their website)
http://www.novaccine.com/pdffiles/Act_HIB_package_insert.pdf
Havrix: the Hepatitis A Vaccine
According to the product insert, there were an enormous number of participants: 32,900, engaged in 60 clinical trials! Which is pretty... interesting. How exactly and why exactly did they choose to do it that way?? At any rate, the information posted for the two principle safety trials (the only ones they include any information about specifically on the p.i.): The first stated it was compared to the Energix B vaccination, the second stated it was compared to Infanrix DTaP vaccination and a conjugatae HiB vaccine (both). Duration of monitoring on the first study was not noted, however in the second study the amount of duration was only 4 days post vaccination via the use of "diary cards" given to the parents.
http://us.gsk.com/products/assets/us_havrix.pdf
Energix B: the Hepatitis B Vaccine
Every trial participant in this clinical and safety trial were 6 years or older! This vaccination is administered to infants 12 hours out of the womb and given regularly on the recommended childhood immunization schedule otherwise from birth through five! Talk about an obtuse methodological error. The vaccine was also compared not to a control but to another vaccination.
http://us.gsk.com/products/assets/us_engerixb.pdf
Prevnar: the Pneumococcal Vaccine
Was tested against another vaccine and not a control (an "investigative" aka experimental, Men C vaccine no less). No specific date of monitoring for adverse reactions was given but the product insert did state "the pre protocol analysis of the primary end point included cases which occured >14 days after the third dose."
http://www.wyeth.com/content/showlabeling.asp?id=134
Menactra: the Meningococcal Vaccine
The vaccination was compared to the Menomune vaccination and not a control. There were 7 days of solicited monitoring post vaccination via "diary cards" included in the 28 days of unsolicited adverse reaction monitoring post vaccination (aka if the parent had something happen to their child they could report it within those 28 days, but nobody would be contacting them after the intial 7 days to find out).
https://www.vaccineshoppe.com/image.cfm?doc_id=8826&image_type=product_pdf
Fluzone: the Influenza Vaccine
Was not compared to a control. Safety study included a total of 31 children (19 children aged 6 to 23 months and 12 children aged 24 to 36 months), that's it! They were given two total doses of vaccines spaced one month apart and local and systemic reactions were only solicited for 3 days post vaccination.
https://www.vaccineshoppe.com/image.cfm?doc_id=10913&image_type=product_pdf
Note: the Rotavirus and Gardasil vaccinations were the only ones that checked out for being placebo controlled and appropriately conducted. Good job guys!
Unfortunately these are two vaccinations designed for totally mild conditions which both admit to a causative association with FATALITY. If it wasn't such a terrible combination, you would think God had a keen sense of humor. The only two appropriately researched vaccinations are the ones made for innocuous conditions and they can cause death in their recipients? Woooow.
If you don't believe me check out the Rotavirus vaccine product insert which concedes to an uncontested causation of death (which is oddly the reason the first rotavirus vaccine got banned, although the manner of death was different... I guess it takes them a while to learn!):
http://www.fda.gov/BiologicsBloodVaccines/Vaccines/ApprovedProducts/ucm133920.htm
Or the Gardasil vaccine product insert which concedes to an uncontested causation of arrhythmia, which can most certainly be fatal, among a VERY long list of debilitating diseases including Asthma, Sepsis, Pancreatic cancer and rheumatoid arthritis.
http://www.merck.com/product/usa/pi_circulars/g/gardasil/gardasil_pi.pdf
The point of this article on safety studies is clear: the next time you get the thought that the FDA or any other governmental entity is absolutely ensuring your safety with it's "rigid" safety testing standards of drugs and pharmaceutical products, please think again! If this is how pathetic the standards are for testing chemicals that are going to be injected into infants bodies is, imagine how "stringent" the standards must be for adult medicines.
Always make sure you look at the product inserts for yourself before consenting to using any pharmaceutical product. There is a laundry list of FDA approved drugs out there that carry more serious adverse reaction risks than the condition they were designed to treat. And never forget, being a smart patient benefits you as well as your physician. Thanks for reading.
Wednesday, October 28, 2009
Global Vaccine Comparison
The United States recommends a total of 48 doses of childhood immunizations before age 6 on the routine childhood immunization schedule. They are as follows:
Birth (12 hours)
Hepatitis B
2 Months
Diphtheria
Tetanus
Pertussis
Polio
HiB
PCV (Pneumococcal)
Rotavirus
Hepatitis B
4 Months
Diphtheria
Tetanus
Pertussis
Polio
HiB
PCV (Pneumococcal)
Rotavirus
6 Months
Diphtheria
Tetanus
Pertussis
Polio
PCV (Pneumococcal)
Rotavirus
Hepatitis B
Influenza
7 Months
Influenza
12-15 Months
HiB
PCV (Pneumococcal)
Measles
Mumps
Rubella
Varicella
Hepatitis A
18 Months
Diptheria
Tetanus
Pertussis
Hepatitis A
Influenza
3 Years
Influenza
4-6 Years
Diptheria
Tetanus
Pertussis
Polio
Measles
Mumps
Rubella
Varicella
Influenza (2)
An additional copy of the routine childhood immunization schedule for verification may be obtained at: http://www.909shot.com/NVIC_poster2(hi-res).pdf
From birth through FIVE however there are typically 36 doses given in the United States. It is easier to compare birth through five because this is the age category the World Health Organization has created. Examing the WHO's information for the top 30 countries for mortality (which may be found by country at: www.who.int/vaccines/globalsummary/immunization/ScheduleResult.cfm) we can see some of the differences in global vaccine strategy and another interesting factor: mortality rate. See also http://fourteenstudies.org/nowwhat.html.
The order goes: Country... # of Mandatory Vaccines
(<5 yrs old).... Mortality Rates per 1,000 Children Under 5 yrs old... Mortality Rate Worldwide Rank
United States 36 7.8 34
Iceland 11...3.9...1
Sweden 11...4.0...2
Singapore 13...4.1... 3
Japan 11... 4.2... 4
Norway 13... 4.4... 5
Finland 12... 4.7... 6
Hong Kong 13... 4.7... 7
Czech Republic 20... 4.8... 8
South Korea (recommended dose info unavailable) 4.8... 9
Switzerland 16...5.1...10
France 17...5.2...11
Spain 20...5.3...12
Belgium 18...5.3...13
Germany 22..5.4...14
Austria 19...5.4...15
Australia 27...5.6...16
Israel 11...5.7...17
Denmark 12...5.8...18
Netherlands 20...5.9...19
Canada 28...5.9...20
United Kingdom 20...6.0...21
Italy 13...6.1...22
Ireland 24...6.2...23
Channel Islands (recommended dose info unavailable) 6.2... 24
Slovenia 14...6.4...25
New Zealand 21...6.4...26
Cuba (recommended dose info unavailable) 6.5...27
Luxembourg 23...6.6...28
Portugal 19...6.6...29
Brunei (recommended dose info unavailable) 6.7...30
Cyprus 23...6.9...31
Malta 14...7.6...32
Croatia 18...7.7...33
Average number of doses of countries with available figure= 18.0!
So here we wind up with some very intriguing information: 30 countries in the world with the best childhood mortality rates, recommend about 20 doses less vaccines from birth through 5 than the United States does, which is 34th in the world for childhood mortality in this age group (pretty terrible considering we're the wealthiest nation on earth isn't it?). Shouldn't all of those extra doses of vaccinations that we're giving our kids make them LESS likely to die? I mean for crying out loud, even Croatia and CUBA are beating us!
Naturally there are a large variety of factors influencing childhood mortality, such as access to health care, environmental pollution, hygiene and sanitation, availability of an uncontaminated water supply and so forth. While the United States certainly has issues with health care access to the middle class, vaccinations are free at any state health department in the country. We have in fact one of the highest childhood vaccination rates on earth with a 97-98% rate of immunization (darn those 3% that aren't vaccinating their kids!) which exceeds herd immunity standards. Furthermore most of the countries on this list do not mandate and enforce vaccinations the way some US states do and the vaccination rate for their countries is typically lower.
So why isn't the rest of the world complying with OUR vaccination schedule? Why are they not giving children 36 vaccines from birth through five, 48 from birth through six, and 69 from birth through eighteen? And how come more of their chilren are not sick and dying as a result? These are viable questions and we should be asking them.
Birth (12 hours)
Hepatitis B
2 Months
Diphtheria
Tetanus
Pertussis
Polio
HiB
PCV (Pneumococcal)
Rotavirus
Hepatitis B
4 Months
Diphtheria
Tetanus
Pertussis
Polio
HiB
PCV (Pneumococcal)
Rotavirus
6 Months
Diphtheria
Tetanus
Pertussis
Polio
PCV (Pneumococcal)
Rotavirus
Hepatitis B
Influenza
7 Months
Influenza
12-15 Months
HiB
PCV (Pneumococcal)
Measles
Mumps
Rubella
Varicella
Hepatitis A
18 Months
Diptheria
Tetanus
Pertussis
Hepatitis A
Influenza
3 Years
Influenza
4-6 Years
Diptheria
Tetanus
Pertussis
Polio
Measles
Mumps
Rubella
Varicella
Influenza (2)
An additional copy of the routine childhood immunization schedule for verification may be obtained at: http://www.909shot.com/NVIC_poster2(hi-res).pdf
From birth through FIVE however there are typically 36 doses given in the United States. It is easier to compare birth through five because this is the age category the World Health Organization has created. Examing the WHO's information for the top 30 countries for mortality (which may be found by country at: www.who.int/vaccines/globalsummary/immunization/ScheduleResult.cfm) we can see some of the differences in global vaccine strategy and another interesting factor: mortality rate. See also http://fourteenstudies.org/nowwhat.html.
The order goes: Country... # of Mandatory Vaccines
(<5 yrs old).... Mortality Rates per 1,000 Children Under 5 yrs old... Mortality Rate Worldwide Rank
United States 36 7.8 34
Iceland 11...3.9...1
Sweden 11...4.0...2
Singapore 13...4.1... 3
Japan 11... 4.2... 4
Norway 13... 4.4... 5
Finland 12... 4.7... 6
Hong Kong 13... 4.7... 7
Czech Republic 20... 4.8... 8
South Korea (recommended dose info unavailable) 4.8... 9
Switzerland 16...5.1...10
France 17...5.2...11
Spain 20...5.3...12
Belgium 18...5.3...13
Germany 22..5.4...14
Austria 19...5.4...15
Australia 27...5.6...16
Israel 11...5.7...17
Denmark 12...5.8...18
Netherlands 20...5.9...19
Canada 28...5.9...20
United Kingdom 20...6.0...21
Italy 13...6.1...22
Ireland 24...6.2...23
Channel Islands (recommended dose info unavailable) 6.2... 24
Slovenia 14...6.4...25
New Zealand 21...6.4...26
Cuba (recommended dose info unavailable) 6.5...27
Luxembourg 23...6.6...28
Portugal 19...6.6...29
Brunei (recommended dose info unavailable) 6.7...30
Cyprus 23...6.9...31
Malta 14...7.6...32
Croatia 18...7.7...33
Average number of doses of countries with available figure= 18.0!
So here we wind up with some very intriguing information: 30 countries in the world with the best childhood mortality rates, recommend about 20 doses less vaccines from birth through 5 than the United States does, which is 34th in the world for childhood mortality in this age group (pretty terrible considering we're the wealthiest nation on earth isn't it?). Shouldn't all of those extra doses of vaccinations that we're giving our kids make them LESS likely to die? I mean for crying out loud, even Croatia and CUBA are beating us!
Naturally there are a large variety of factors influencing childhood mortality, such as access to health care, environmental pollution, hygiene and sanitation, availability of an uncontaminated water supply and so forth. While the United States certainly has issues with health care access to the middle class, vaccinations are free at any state health department in the country. We have in fact one of the highest childhood vaccination rates on earth with a 97-98% rate of immunization (darn those 3% that aren't vaccinating their kids!) which exceeds herd immunity standards. Furthermore most of the countries on this list do not mandate and enforce vaccinations the way some US states do and the vaccination rate for their countries is typically lower.
So why isn't the rest of the world complying with OUR vaccination schedule? Why are they not giving children 36 vaccines from birth through five, 48 from birth through six, and 69 from birth through eighteen? And how come more of their chilren are not sick and dying as a result? These are viable questions and we should be asking them.
Pneumococcal Vaccines and Serotype Replacement
Meningitis vaccinations may possibly be the only vaccinations that this author would consider administering to her own children, knowing how frightening and dangerous meningitis is. Unfortunately, like HiB, this Prevnar (pneumococcal) vaccine has simply resulted in serotype replacement with equally virulent NVS's (non vaccine serotypes). It's amazing to me that doctors want us to risk Asthma, Pneumonia, Congestive Heart Failure, Sepsis, and even Death (see http://www.wyeth.com/content/showlabeling.asp?id=134 for product insert admiting causation to these severe adverse reactions) when the only thing you're getting in return is a switcheroo for an equally terrible disease.
References of Pneumococcal Serotype Replacement Documentation:
"While the rates of all resistant diseases caused by the vaccines serotype fell 87 precent, the rates of serotype 19A disease, a deadly type in the very young, rose by 315 percent between 1999 and 2004."
-Kyaw MH, "Effect of the introduction of the pneumococcal conjugate vaccine on drug resistant streptopoccus pneuomniae"; New England Journal of Medicine, April 2006
"During the post licensure period, there were significant decreases in the incidence of pneumococcal bacteremia caused by vaccine serotypes; however, rate of penicillin resistance and bacteremia due to non-vaccine related serotypes increased."
-Steenhoof AD, Shann SS, Emergence of vaccine related pneomococcal serotypes as a cause of bacteremia, The Childrens Hospital of Philadelphia, Clinical Infectious Diseases, April 2006
-Farrell DJ; "Increased antimicrobial resistance among non vaccine serotypes of Streptococcus pneumoniae in the pediatric population after the introduction of 7 valent pneumococcal vaccine in the United States"; Pediatr Infect Dis J. 2007 Feb;26(2):123-8
CONCLUSIONS: In Dallas , heptavalent pneumococcal conjugate vaccine reduced the incidence of IPD from 1999 to 2005 by reducing the incidence of vaccine-type disease. NVT serotypes, particularly 19A, were prevalent and more resistant to antimicrobials in 2004 and 2005
-Messina AF, "Impact of the pneumococcal conjugate vaccine on serotype distribution and antimicrobial resistance of invasive streptococcus pneumoniae isolates in Dallas, TX children from 1999 through 2005."; Pediatr Infect Dis J. 2007 June;26(6)461-7
CONCLUSIONS: Three years after the introduction of pneumococcal conjugate vaccine for universal administration to children less than 2 in Massachusetts, a significant increase in invasive disease due to serotype 19A was observed. Although MLST 199 remains the most frequent sequence type among invasive isolates (of 19A), a multidrug-resistant sequence type, not previously identified in Massachusetts , has become an important cause of invasive disease. Further surveillance of the changing ecology of S. pneumoniae is necessary as a 4-year time period is not sufficient to fully evaluate the impact of PCV of pneumococcal infections.
-Pelton SI; "Emergence of 19A as virulent and multi-drug resistant Pneumococcus in Massachusetts following universal immunization with pneumoccocal conjugate vaccine."; Pediatr Infect Dis. 2007 June;26(6)468-72
BACKGROUND: The introduction of the 7-valent conjugate pneumococcal vaccine (PCV7) in children may result in serotype replacement.
CONCLUSION: Serotype 19A is, at present, the most important cause of IPD by replacement serotypes, and it is increasingly drug resistant. CC199 is the predominant CC among type 19A serotypes in children <5 years old. Our data suggest that some of the increase in rates of infection with serotype 19A may be due to serotype switching within certain vaccine type strains.
-Pai R; "Postvaccine genetic structure of Streptococcus pneumoniae serotype 19A from children in the United States." J Infect Dis. 2005 Dec 1;192(11):1988-95
References of Pneumococcal Serotype Replacement Documentation:
"While the rates of all resistant diseases caused by the vaccines serotype fell 87 precent, the rates of serotype 19A disease, a deadly type in the very young, rose by 315 percent between 1999 and 2004."
-Kyaw MH, "Effect of the introduction of the pneumococcal conjugate vaccine on drug resistant streptopoccus pneuomniae"; New England Journal of Medicine, April 2006
"During the post licensure period, there were significant decreases in the incidence of pneumococcal bacteremia caused by vaccine serotypes; however, rate of penicillin resistance and bacteremia due to non-vaccine related serotypes increased."
-Steenhoof AD, Shann SS, Emergence of vaccine related pneomococcal serotypes as a cause of bacteremia, The Childrens Hospital of Philadelphia, Clinical Infectious Diseases, April 2006
-Farrell DJ; "Increased antimicrobial resistance among non vaccine serotypes of Streptococcus pneumoniae in the pediatric population after the introduction of 7 valent pneumococcal vaccine in the United States"; Pediatr Infect Dis J. 2007 Feb;26(2):123-8
CONCLUSIONS: In Dallas , heptavalent pneumococcal conjugate vaccine reduced the incidence of IPD from 1999 to 2005 by reducing the incidence of vaccine-type disease. NVT serotypes, particularly 19A, were prevalent and more resistant to antimicrobials in 2004 and 2005
-Messina AF, "Impact of the pneumococcal conjugate vaccine on serotype distribution and antimicrobial resistance of invasive streptococcus pneumoniae isolates in Dallas, TX children from 1999 through 2005."; Pediatr Infect Dis J. 2007 June;26(6)461-7
CONCLUSIONS: Three years after the introduction of pneumococcal conjugate vaccine for universal administration to children less than 2 in Massachusetts, a significant increase in invasive disease due to serotype 19A was observed. Although MLST 199 remains the most frequent sequence type among invasive isolates (of 19A), a multidrug-resistant sequence type, not previously identified in Massachusetts , has become an important cause of invasive disease. Further surveillance of the changing ecology of S. pneumoniae is necessary as a 4-year time period is not sufficient to fully evaluate the impact of PCV of pneumococcal infections.
-Pelton SI; "Emergence of 19A as virulent and multi-drug resistant Pneumococcus in Massachusetts following universal immunization with pneumoccocal conjugate vaccine."; Pediatr Infect Dis. 2007 June;26(6)468-72
BACKGROUND: The introduction of the 7-valent conjugate pneumococcal vaccine (PCV7) in children may result in serotype replacement.
CONCLUSION: Serotype 19A is, at present, the most important cause of IPD by replacement serotypes, and it is increasingly drug resistant. CC199 is the predominant CC among type 19A serotypes in children <5 years old. Our data suggest that some of the increase in rates of infection with serotype 19A may be due to serotype switching within certain vaccine type strains.
-Pai R; "Postvaccine genetic structure of Streptococcus pneumoniae serotype 19A from children in the United States." J Infect Dis. 2005 Dec 1;192(11):1988-95
HiB Vaccine and Serotype Replacement
Hib vaccine has undoubtedly caused a vast decrease in the incidence of type b Haemophilus Influenza. However, this decrease in type B has been offset by a significant increase in non type b forms of Haemophilus Influenza. Recommending patients to take the risk of neurological disorders, encephalopathy, permanent brain damage and anaphylaxis (plus an increased risk of HiB for one week post vaccination), all of which are conceeded as causal serious adverse reactions on the product insert(http://www.novaccine.com/pdffiles/Act_HIB_package_insert.pdf).... for the sake of their child probably just ending up with another serotype of the same form of meningitis, is logically unstable and ethically questionable.
References of Serotype Replacement Documentation:
"In addition to the proportional increasei n cases of non type b Haemophilus influenzae disease in the post H influenzae type b vaccine era, the incident of invasive H influenzae disease was found to be approaching the rates of H Influenzae type b disease that were documented in the pre vaccine period."
Tsang RS; "Characterization of invasive Haemophilus influenza disease in Manitoba Canada, 2000-2006: invasive disease due to non type b strains." Clin Infect Dis. 2007 June 15;44(12):1611-4
--------------------------------------------------------------------------------
"Non-capsulate H influenzae isolates have shown an increase in annual attack rate (for all ages) from 0.25 cases per 100000 population in 1990-1 (45 cases recorded) to 0.37 in 1993-4 (67 cases). The total number of recorded cases of non-type b infections (non-capsulate and other serotypes: 75 cases) exceeded the number of cases of H influenzae type b (50 cases) in 1993-4. These increases demonstrate a sustained trend, approaching significance for non-capsulate infections during 1993-4 (P=0.066)."
Ruth M Hargreaves, Mary P E Slack,"Changing patterns of invasive Haemophilus influenzae disease in England and Wales after introduction of the Hib vaccination programme"; BMJ 1996;312:160-161 (20 January)
-------------------------------------------------------------
Waggoner-Fountain LA; "The emergence of Haemophilus influenzae types e and f as significant pathogens."; Clin Infect Dis 1995 Nov;21(5):1322-4
-------------------------------------------------------------------------
Korgenski EK, "Invasive serotype a Haeomophilus influnzae infections with a virulence genotype resembing Haemophilus influenzae type b: emerging pathogen in the vaccine era?"; 1: Pediatrics. 2001 Jul;108(1): E18
-----------------------------------------------------------------------
Ribeiro GS, "Prevention of Haemophilus influenz type b (Hib) meningitis and emergence of serotype replacement with type a strains after introduction of the HiB imunization in Brazil." J Infect Dis. 2003 Jan 1;187(1):109-16
--------------------------------------------------------------
Heath PT, "Non type b Haemophilus influenzae disease: clinical and epidemiologic characteristics in the Haemophilus influenzae type b vaccine era." Pediatr Infect Dis J. 2001 Mar;20(3):300-5
-------------------------------------------------------------------
Mulhelmann K, "Molecular characteristics of Haemophilus influenzae causing invasive disease during the period of vaccination in Switzerland: analysis of isolated strains between 1986 and 1993." J Clin Microbiol. 1996 Mar;34(3)560-3
------------------------------------------------------------------------------
Campos J; "Analysis of invasive Haemophilus influenzae infections after extensive vaccination against H. influenzae type b". J Clin Microbiol. 2004 Feb;42(2):524-9
References of Serotype Replacement Documentation:
"In addition to the proportional increasei n cases of non type b Haemophilus influenzae disease in the post H influenzae type b vaccine era, the incident of invasive H influenzae disease was found to be approaching the rates of H Influenzae type b disease that were documented in the pre vaccine period."
Tsang RS; "Characterization of invasive Haemophilus influenza disease in Manitoba Canada, 2000-2006: invasive disease due to non type b strains." Clin Infect Dis. 2007 June 15;44(12):1611-4
--------------------------------------------------------------------------------
"Non-capsulate H influenzae isolates have shown an increase in annual attack rate (for all ages) from 0.25 cases per 100000 population in 1990-1 (45 cases recorded) to 0.37 in 1993-4 (67 cases). The total number of recorded cases of non-type b infections (non-capsulate and other serotypes: 75 cases) exceeded the number of cases of H influenzae type b (50 cases) in 1993-4. These increases demonstrate a sustained trend, approaching significance for non-capsulate infections during 1993-4 (P=0.066)."
Ruth M Hargreaves, Mary P E Slack,"Changing patterns of invasive Haemophilus influenzae disease in England and Wales after introduction of the Hib vaccination programme"; BMJ 1996;312:160-161 (20 January)
-------------------------------------------------------------
Waggoner-Fountain LA; "The emergence of Haemophilus influenzae types e and f as significant pathogens."; Clin Infect Dis 1995 Nov;21(5):1322-4
-------------------------------------------------------------------------
Korgenski EK, "Invasive serotype a Haeomophilus influnzae infections with a virulence genotype resembing Haemophilus influenzae type b: emerging pathogen in the vaccine era?"; 1: Pediatrics. 2001 Jul;108(1): E18
-----------------------------------------------------------------------
Ribeiro GS, "Prevention of Haemophilus influenz type b (Hib) meningitis and emergence of serotype replacement with type a strains after introduction of the HiB imunization in Brazil." J Infect Dis. 2003 Jan 1;187(1):109-16
--------------------------------------------------------------
Heath PT, "Non type b Haemophilus influenzae disease: clinical and epidemiologic characteristics in the Haemophilus influenzae type b vaccine era." Pediatr Infect Dis J. 2001 Mar;20(3):300-5
-------------------------------------------------------------------
Mulhelmann K, "Molecular characteristics of Haemophilus influenzae causing invasive disease during the period of vaccination in Switzerland: analysis of isolated strains between 1986 and 1993." J Clin Microbiol. 1996 Mar;34(3)560-3
------------------------------------------------------------------------------
Campos J; "Analysis of invasive Haemophilus influenzae infections after extensive vaccination against H. influenzae type b". J Clin Microbiol. 2004 Feb;42(2):524-9
Tuesday, October 27, 2009
The Polio Vaccine: Greatest Medical Miracle Of Our Time?
Was the Polio vaccine really the greatest medical miracle of our time, or was it simply the most elaborate cover up?
*CDC Statistic: Before Polio vaccine was available, 13,000 to 20,000 cases of paralytic Polio were reported each year in the U.S.
www.cdc.gov/vaccines/vac-gen/whatifstop.htm
*Response: Paralytic Polio was pre-determined to decrease down to essentially nill when the reporting standards were changed in 1955. The standards of reporting paralytic Polio changed from only 24 hours of symptoms to more than 60 days of symptoms, which virtually eliminated paralytic Polio from statistics, as paralytic Polio typically resolves within weeks, not months. Generic Poliomyelitis was also removed from statistics via “elegant administrative moves”, which also began in 1955, when the a change in medical reporting standards occurred that now required Poliomyelitis to be reported under different names, mainly viral or aseptic meningits, or coxsackie virus.
Sources:
Hearings Before the Committee on Interstate and Foreign Commerce, House of Representatives, 87th Congress, 2nd Session on HR 10541; May 1962: 94-112
Catherine Diodati MA; Immunization History Ethics Law and Health, pg. 116
Neil Z Miller: The polio vaccine: a critical assessment of its arcane history, efficacy, and long term health related consequences, 2004
Bulletin of the American Association of Public Health Physicians; 1954
Proceedings of the 120th Annual Meeting of the Illinois Medical Society; Illinois Medical Journal; August 1960
"Data shown in this report are confined to paralytic poliomyelitis only. It may be noted that the Dominion Council of Health at it's 74th meeting in October 1958 recommended that for the purposes of national reporting and statistics the term non paralytic poliomyelitis be replaced by 'meningitis, viral or aseptic' with the specific viruses shown where known."
-The Dominion Bureau of Statistics Official Bulletin, Poliomyelitis Trends, 1958; June 1959 (Canada)
"Go to your medical library and ask to see the United States Polio Surveillance Units bulletins, from 1955 to 1970. They will be listed as 'missing'. Every single medical library in the USA and New Zealand has them listed as 'missing'. There is only one place you can see them as far as I know, and that is the AMA library, and they are listed as having top security clearance requirements to see. Why might this be? When he was alive, Dr. Ratner had copies of them in his home. He gave me many years' data that I wanted. They clearly showed that from the inception of the Salk vaccine to it's discontinuation, the vaccine had minus efficacy and was actually causing more Polio in the vaccinated than the unvaccinated. Any studious person looking at government stats in retrospect would be able to easily see that the political and media canonization of Salk and his vaccine was a mirage of duplicity upon duplicity."
-Hilary Butler MD (2009 April)
The question of the iron lung: if the Polio vaccine never eradicated Polio, what happened to all of those iron lungs?
An appropriate common sense question with an appropriate common sense answer: iron lungs were already on their way out when the Polio vaccine was being introduced. "The drinker", aka iron lung, was a negative pressure ventilator and was replaced by positive pressure ventilation as early as 1952 in the United States.
*CDC Statistic: As a result of global eradication efforts, the number of cases has decreased from 350,000 cases in 125 countries in 1988 to 2,000 cases in 17 countries in 2006.
www.cdc.gov/vaccines/vac-gen/whatifstop.htm
*Response: the reasoning for the radical “decrease” in Polio from 1988 to 2006 is identical to the reasoning for the original decrease in 1955: changes in the definition of the disease, only this time on an international platform. Poliomyelitis now operates under such terminology as “Guillain Barre Syndrome”, “Chinese Paralytic Syndrome”, “Chronic Fatigue Syndrome”, and so on. There exists, in fact, a shockingly long list of polio-identical or nearly-exact illnesses in the world community. In fact, as early as 1950, more than 170 of these diseases were documented by Ralf R. Scobey, who was the president of the Poliomyeltis Research Institute Inc., at the time and are available for viewing in the Archives of Pediatrics in Syracus, New York (1946-1953).
See also:
-William Campbell Douglass, MD: "chronic fatigue syndrome: the hidden polio epidemic", Second Opinion Newsletter
An Excellent Reference on the Many Names of Polio:
www.whale.to/vaccine/polio1.html
*Informed Citizens Against Vaccination claims that the eradication of “Polio” at the hands of the World Health Organization (WHO) has been successful, if one considers simply re-naming a disease and changing its reporting standards as sufficient. We, however, do not. The real problems that are creating such massive epidemics of disease across the world community are not being addressed. If we are going to find a true cure for poliomyelitis at some point, the entire international community is going to have to experience a major wake up call that the vaccinations are NOT it.
*CDC Statistic: Before Polio vaccine was available, 13,000 to 20,000 cases of paralytic Polio were reported each year in the U.S.
www.cdc.gov/vaccines/vac-gen/whatifstop.htm
*Response: Paralytic Polio was pre-determined to decrease down to essentially nill when the reporting standards were changed in 1955. The standards of reporting paralytic Polio changed from only 24 hours of symptoms to more than 60 days of symptoms, which virtually eliminated paralytic Polio from statistics, as paralytic Polio typically resolves within weeks, not months. Generic Poliomyelitis was also removed from statistics via “elegant administrative moves”, which also began in 1955, when the a change in medical reporting standards occurred that now required Poliomyelitis to be reported under different names, mainly viral or aseptic meningits, or coxsackie virus.
Sources:
Hearings Before the Committee on Interstate and Foreign Commerce, House of Representatives, 87th Congress, 2nd Session on HR 10541; May 1962: 94-112
Catherine Diodati MA; Immunization History Ethics Law and Health, pg. 116
Neil Z Miller: The polio vaccine: a critical assessment of its arcane history, efficacy, and long term health related consequences, 2004
Bulletin of the American Association of Public Health Physicians; 1954
Proceedings of the 120th Annual Meeting of the Illinois Medical Society; Illinois Medical Journal; August 1960
"Data shown in this report are confined to paralytic poliomyelitis only. It may be noted that the Dominion Council of Health at it's 74th meeting in October 1958 recommended that for the purposes of national reporting and statistics the term non paralytic poliomyelitis be replaced by 'meningitis, viral or aseptic' with the specific viruses shown where known."
-The Dominion Bureau of Statistics Official Bulletin, Poliomyelitis Trends, 1958; June 1959 (Canada)
"Go to your medical library and ask to see the United States Polio Surveillance Units bulletins, from 1955 to 1970. They will be listed as 'missing'. Every single medical library in the USA and New Zealand has them listed as 'missing'. There is only one place you can see them as far as I know, and that is the AMA library, and they are listed as having top security clearance requirements to see. Why might this be? When he was alive, Dr. Ratner had copies of them in his home. He gave me many years' data that I wanted. They clearly showed that from the inception of the Salk vaccine to it's discontinuation, the vaccine had minus efficacy and was actually causing more Polio in the vaccinated than the unvaccinated. Any studious person looking at government stats in retrospect would be able to easily see that the political and media canonization of Salk and his vaccine was a mirage of duplicity upon duplicity."
-Hilary Butler MD (2009 April)
The question of the iron lung: if the Polio vaccine never eradicated Polio, what happened to all of those iron lungs?
An appropriate common sense question with an appropriate common sense answer: iron lungs were already on their way out when the Polio vaccine was being introduced. "The drinker", aka iron lung, was a negative pressure ventilator and was replaced by positive pressure ventilation as early as 1952 in the United States.
*CDC Statistic: As a result of global eradication efforts, the number of cases has decreased from 350,000 cases in 125 countries in 1988 to 2,000 cases in 17 countries in 2006.
www.cdc.gov/vaccines/vac-gen/whatifstop.htm
*Response: the reasoning for the radical “decrease” in Polio from 1988 to 2006 is identical to the reasoning for the original decrease in 1955: changes in the definition of the disease, only this time on an international platform. Poliomyelitis now operates under such terminology as “Guillain Barre Syndrome”, “Chinese Paralytic Syndrome”, “Chronic Fatigue Syndrome”, and so on. There exists, in fact, a shockingly long list of polio-identical or nearly-exact illnesses in the world community. In fact, as early as 1950, more than 170 of these diseases were documented by Ralf R. Scobey, who was the president of the Poliomyeltis Research Institute Inc., at the time and are available for viewing in the Archives of Pediatrics in Syracus, New York (1946-1953).
See also:
-William Campbell Douglass, MD: "chronic fatigue syndrome: the hidden polio epidemic", Second Opinion Newsletter
An Excellent Reference on the Many Names of Polio:
www.whale.to/vaccine/polio1.html
*Informed Citizens Against Vaccination claims that the eradication of “Polio” at the hands of the World Health Organization (WHO) has been successful, if one considers simply re-naming a disease and changing its reporting standards as sufficient. We, however, do not. The real problems that are creating such massive epidemics of disease across the world community are not being addressed. If we are going to find a true cure for poliomyelitis at some point, the entire international community is going to have to experience a major wake up call that the vaccinations are NOT it.
The Mucosal Systems Role In Immunity
In previous posts regarding the antibody theory of innoculation being misleading (some may even consider erroneous); the follow up topic for discussion was a must: the mucosal system and it's role in conferring humoral immunity, as the direct injection of the pathogen into the bloodstream, a completely unnatural portal for infectious disease conference, is vaccine sciences' second biggest blunder.
For education and edification on the mucosal system and mucosal IgA in particular:
What is Mucosal Secretory IgA and how is it important?
*"All vaccines, with the exception of the OPV (oral polio vaccine), are injected directly into the bloodstream, bypassing the mucosal immune system known as the secretory IgA. The secretory IgA is the first in a series of defensive levels within the immune system. It serves as a buffer, filtering microbes so that the impact of these invading organisms is greatly reduced once it reaches the bloodstream. The IgA allows the antigen to be removed in the same manner in which it arrived- through the mucosal barrier- by sneezing, coughing and sweating. So a vaccine that has been injected gives the body no warning, no chance to recognize, duplicate or defend itself against future challenge from typical antigens."
-Dr. Robert Mendelsohn, How to Raise a Healthy Child in Spite of Your Doctor; Ballantine Books
*The Humoral Immune Response (HIR) is the aspect of immunity that is mediated by secreted antibodies (as opposed to cell-mediated immunity which involves T lymphocytes) produced in the cells of the B lymphocyte lineage (B cell). Secreted antibodies bind to antigens on the surfaces of invading microbes (such as viruses or bacteria), which flags them for destruction.Immunoglobulin A (IgA) is an antibody playing a critical role in mucosal immunity.
More IgA is produced in mucosal linings than all other types of antibody combined. Because it is resistant to degradation by enzymes, secretory IgA can survive in harsh environments such as the digestive and respiratory tracts, to provide protection against microbes that multiply in body
secretions.
-http://en.wikipedia.org/wiki/Humoral_immunity
*What the promoters of vaccination failed to realize is that the respiratory tract of ALL mammals (since animals are just as devastated by these inoculations with disease as are humans) contain secretory IgA (an antibody which initiates the natural God given immune response) within the respiratory tract mucosa. Bypassing this mucosal aspect of the immune system by directly injecting organisms into the bloodstream leads to a corruption in the immune system itself. As a result, the pathogenic viruses or bacteria cannot be eliminated by the immune system and remain in the body, where they will further grow and/or mutate as the individual is exposed to ever more antigens and toxins in the environment which continue to assault the immune system.
Inoculations - By Rebecca Carley, M.D. 01-29-2005 Court Qualified Expert in VIDS and Legal Abuse Syndrome
*SIgA serves as the first line of defense against microorganisms through a mechanism called immune exclusion. In terms of humoral immunity at mucosal surfaces, SIgA appears thus to combine properties of a neutralizing agent (immune exclusion) and of a mucosal immunopotentiator inducing effector immune responses in a noninflammatory context favorable to preserve local homeostasis of the gastrointestinal tract.
In humans, mucosal surfaces of the gut, the airways, the urogenital tracts, and the ducts of all exocrine glands are lined by epithelial layers that form tight barriers separating a rapidly changing external environment from a highly regulated internal compartment. Due to the vast surface they cover, these vulnerable cellular barriers are the most frequent portals of entry for microorganisms and exogenous materials. Mucosal surfaces are endowed with powerful defense mechanisms, which selectively process harmful or innocuous Ags to guarantee local homeostasis.
The Journal of Immunology, 2007, 178: 27-32.Roundtrip Ticket for Secretory IgA: Role in Mucosal Homeostasis?1 Blaise Corthésy2
--------------------------------------------------------------
If systemic (injected) vaccinations were so effective at providing immunity, modern allopathic medicine would not be scrambling for a mucosal alternative. Here are some examples of the search for a mucosal alternative to current vaccine implementations:
Marian R. Neutra1,2 & Pamela A. Kozlowski1 Mucosal vaccines: the promise and the challenge Nature Reviews Immunology 6, 148-158 (February 2006)
Author affiliations
1. GI Cell Biology Research Laboratory, Children's Hospital and Department of Pediatrics, Harvard Medical School, Boston, Massachusetts 02115, USA.
2. Children's Hospital, Enders 720, 300 Longwood Avenue, Boston, Massachusetts 02115, USA.
Mucosal vaccination has several advantages over parenteral vaccination, including the induction of an immune response at the site of administration. Furthermore, immunization at one mucosal site can induce specific responses at distant sites, providing protective mucosal immunity. In addition to local responses against mucosally-acquired pathogens, mucosal vaccines induce systemic immunity, including humoral and cell-mediated responses. The administration of mucosal vaccines does not require the use of needles, increasing vaccine compliance, reducing logistical burden, and minimizing the risks of blood transmissible infections.
Yuki, Yoshikazu; Kiyono, Hiroshi Mucosal vaccines: novel advances in technology and delivery; Expert Review of Vaccines, Volume 8, Number 8, August 2009 , pp. 1083-1097(15)
http://www.scq.ubc.ca/mucosal-immunity-and-vaccines/
(extremely interesting and informative article on mucosal immunity!)
http://www.grandchallenges.org/ImproveVaccines/Challenges/NeedleFreeDelivery/Pages/targetedtechnology.aspx
University of California, Riverside, Dr. David Lo
http://www.socmucimm.org/index.php?option=com_content&task=view&id=41&Itemid=65
Plenary Session: Progress in Mucosal Vaccines
Chair: Ken Beagley, PhD, Queensland University of Technology•
Mucosal Adjuvants for Vaccines, Nils Lycke, MD, PhD, University of Goteberg•
IgG and Mucosal Immunity, John B. Robbins, MD, National Institutes of Health•
Rotaviral Vaccination, Harry Greenberg, MD, Stanford University•
Protection Against HIV in the Urogenital Tract, Robin J. Shattock, MD, University of London- St. George’s•
Rice-based Vaccines: New Generation of Mucosal Vaccine, Hiroshi Kiyono, DDS, PhD, University of Tokyo
(The NIH and Stanford included giving lectures on the emerging field of mucosal vaccination).
-------------------------------------------------------------
"Capable of inducing antigen-specific immune responses in both systemic and mucosal compartments without the use of syringe and needle, mucosal vaccination is considered ideal for the global control of infectious diseases."
http://www.pnas.org/content/104/26/10986.abstract
Jiri Mestecky; Perspectives on Mucosal Vaccines: Is Mucosal Tolerance a Barrier?; The Journal of Immunology, 2007, 179, 5633 -5638
http://www.brown.edu/Courses/Bio_160/handouts/feb23.pdf
Why Mucosal Immunization?
• Mucosal surface is major portal of entry for pathogens
• Mucosa contains highest concentration of lymphocytes
6 x 1010 antibody-forming cells in mucosa-associated
lymphoid tissue (MALT)
versus
2.5 x 1010 lymphocytes in lymphoid organs
• Mucosal immunization
- mucosal immunity
- systemic immunity
- prevents infection
Systemic immunization:
- no mucosal immunity
- resolves infection before disease develops
An example given by this Harvard PhD on the benefits of mucosl vaccination for pertussis in comparison to injected: Bordetella pertussis
Parenteral Vaccination
Humans
Immunity diminishes in early adulthood
Only IgG is detected in nasal secretions
Mice
Only IgG is detected in respiratory tract
Natural Infection/ Mucosal Vaccination
Humans
Natural infection = longterm immunity
High titers of specific IgG and IgA in nasal secretions
Mice
Mucosal vaccination generates specific IgG and IgA in respiratory tract
---------------------------------------------------
Authors personal contestations to the development of mucosal vaccinations:
The admittance and pursuing of an alternative to systemic vaccinations is a huge step forward for the movement of vaccine awareness! I am certainly not one to shy away from that. However, the OPV (Oral Polio Vaccine), a mucosal vaccination, has been banned in the western hemisphere and many other parts of the world because it causes provocation poliomyelitis (has in fact caused a large number of cases of Paralytic Polio in India and Africa where it is still being used... because it's too dangerous for us but not for the pharma companies to sell or give away to starving children in developing countries). There are also the flu mist vaccines which go through the nasal mucosal portals, yet carry a risk of neurological disease and alzheimers (among other things), a much greater risk than the risk of the flu itself. So as far as the safety factor is concerned, mucosal vaccines may not be much of an improvement, if any. In terms of effectiveness, however, I remain optimistic and open minded about what mucosal vaccinations may potentially accomplish.
An additional thought is that the concept of stopping children from getting mild and innocuous childhood illnesses that build the immune system in place of supporting nutrition and Vitamin D supplementation is not something I like to support. The theory that perfectly healthy children need drugs and chemicals in their bodies is absolute nonsense, especially when the concept of "they must risking getting such and such frightening diseases so they won't get this other frightening disease" comes into play.
It's a fantastic thing that we are learning more about the complexities of the human immune systems and the role they play in our health; but let's not use it as an excuse to encourage our patients to leave parental responsibility (nutrition, exercise, etc) on the byway because we want to take the lazy road and just inject them with something instead. As any physician knows there is no "automatic" attainment of good health and a strong immune system, the maintaining and developing of such is something that must become a part of our daily lives and rituals.
For education and edification on the mucosal system and mucosal IgA in particular:
What is Mucosal Secretory IgA and how is it important?
*"All vaccines, with the exception of the OPV (oral polio vaccine), are injected directly into the bloodstream, bypassing the mucosal immune system known as the secretory IgA. The secretory IgA is the first in a series of defensive levels within the immune system. It serves as a buffer, filtering microbes so that the impact of these invading organisms is greatly reduced once it reaches the bloodstream. The IgA allows the antigen to be removed in the same manner in which it arrived- through the mucosal barrier- by sneezing, coughing and sweating. So a vaccine that has been injected gives the body no warning, no chance to recognize, duplicate or defend itself against future challenge from typical antigens."
-Dr. Robert Mendelsohn, How to Raise a Healthy Child in Spite of Your Doctor; Ballantine Books
*The Humoral Immune Response (HIR) is the aspect of immunity that is mediated by secreted antibodies (as opposed to cell-mediated immunity which involves T lymphocytes) produced in the cells of the B lymphocyte lineage (B cell). Secreted antibodies bind to antigens on the surfaces of invading microbes (such as viruses or bacteria), which flags them for destruction.Immunoglobulin A (IgA) is an antibody playing a critical role in mucosal immunity.
More IgA is produced in mucosal linings than all other types of antibody combined. Because it is resistant to degradation by enzymes, secretory IgA can survive in harsh environments such as the digestive and respiratory tracts, to provide protection against microbes that multiply in body
secretions.
-http://en.wikipedia.org/wiki/Humoral_immunity
*What the promoters of vaccination failed to realize is that the respiratory tract of ALL mammals (since animals are just as devastated by these inoculations with disease as are humans) contain secretory IgA (an antibody which initiates the natural God given immune response) within the respiratory tract mucosa. Bypassing this mucosal aspect of the immune system by directly injecting organisms into the bloodstream leads to a corruption in the immune system itself. As a result, the pathogenic viruses or bacteria cannot be eliminated by the immune system and remain in the body, where they will further grow and/or mutate as the individual is exposed to ever more antigens and toxins in the environment which continue to assault the immune system.
Inoculations - By Rebecca Carley, M.D. 01-29-2005 Court Qualified Expert in VIDS and Legal Abuse Syndrome
*SIgA serves as the first line of defense against microorganisms through a mechanism called immune exclusion. In terms of humoral immunity at mucosal surfaces, SIgA appears thus to combine properties of a neutralizing agent (immune exclusion) and of a mucosal immunopotentiator inducing effector immune responses in a noninflammatory context favorable to preserve local homeostasis of the gastrointestinal tract.
In humans, mucosal surfaces of the gut, the airways, the urogenital tracts, and the ducts of all exocrine glands are lined by epithelial layers that form tight barriers separating a rapidly changing external environment from a highly regulated internal compartment. Due to the vast surface they cover, these vulnerable cellular barriers are the most frequent portals of entry for microorganisms and exogenous materials. Mucosal surfaces are endowed with powerful defense mechanisms, which selectively process harmful or innocuous Ags to guarantee local homeostasis.
The Journal of Immunology, 2007, 178: 27-32.Roundtrip Ticket for Secretory IgA: Role in Mucosal Homeostasis?1 Blaise Corthésy2
--------------------------------------------------------------
If systemic (injected) vaccinations were so effective at providing immunity, modern allopathic medicine would not be scrambling for a mucosal alternative. Here are some examples of the search for a mucosal alternative to current vaccine implementations:
Marian R. Neutra1,2 & Pamela A. Kozlowski1 Mucosal vaccines: the promise and the challenge Nature Reviews Immunology 6, 148-158 (February 2006)
Author affiliations
1. GI Cell Biology Research Laboratory, Children's Hospital and Department of Pediatrics, Harvard Medical School, Boston, Massachusetts 02115, USA.
2. Children's Hospital, Enders 720, 300 Longwood Avenue, Boston, Massachusetts 02115, USA.
Mucosal vaccination has several advantages over parenteral vaccination, including the induction of an immune response at the site of administration. Furthermore, immunization at one mucosal site can induce specific responses at distant sites, providing protective mucosal immunity. In addition to local responses against mucosally-acquired pathogens, mucosal vaccines induce systemic immunity, including humoral and cell-mediated responses. The administration of mucosal vaccines does not require the use of needles, increasing vaccine compliance, reducing logistical burden, and minimizing the risks of blood transmissible infections.
Yuki, Yoshikazu; Kiyono, Hiroshi Mucosal vaccines: novel advances in technology and delivery; Expert Review of Vaccines, Volume 8, Number 8, August 2009 , pp. 1083-1097(15)
http://www.scq.ubc.ca/mucosal-immunity-and-vaccines/
(extremely interesting and informative article on mucosal immunity!)
http://www.grandchallenges.org/ImproveVaccines/Challenges/NeedleFreeDelivery/Pages/targetedtechnology.aspx
University of California, Riverside, Dr. David Lo
http://www.socmucimm.org/index.php?option=com_content&task=view&id=41&Itemid=65
Plenary Session: Progress in Mucosal Vaccines
Chair: Ken Beagley, PhD, Queensland University of Technology•
Mucosal Adjuvants for Vaccines, Nils Lycke, MD, PhD, University of Goteberg•
IgG and Mucosal Immunity, John B. Robbins, MD, National Institutes of Health•
Rotaviral Vaccination, Harry Greenberg, MD, Stanford University•
Protection Against HIV in the Urogenital Tract, Robin J. Shattock, MD, University of London- St. George’s•
Rice-based Vaccines: New Generation of Mucosal Vaccine, Hiroshi Kiyono, DDS, PhD, University of Tokyo
(The NIH and Stanford included giving lectures on the emerging field of mucosal vaccination).
-------------------------------------------------------------
"Capable of inducing antigen-specific immune responses in both systemic and mucosal compartments without the use of syringe and needle, mucosal vaccination is considered ideal for the global control of infectious diseases."
http://www.pnas.org/content/104/26/10986.abstract
Jiri Mestecky; Perspectives on Mucosal Vaccines: Is Mucosal Tolerance a Barrier?; The Journal of Immunology, 2007, 179, 5633 -5638
http://www.brown.edu/Courses/Bio_160/handouts/feb23.pdf
Why Mucosal Immunization?
• Mucosal surface is major portal of entry for pathogens
• Mucosa contains highest concentration of lymphocytes
6 x 1010 antibody-forming cells in mucosa-associated
lymphoid tissue (MALT)
versus
2.5 x 1010 lymphocytes in lymphoid organs
• Mucosal immunization
- mucosal immunity
- systemic immunity
- prevents infection
Systemic immunization:
- no mucosal immunity
- resolves infection before disease develops
An example given by this Harvard PhD on the benefits of mucosl vaccination for pertussis in comparison to injected: Bordetella pertussis
Parenteral Vaccination
Humans
Immunity diminishes in early adulthood
Only IgG is detected in nasal secretions
Mice
Only IgG is detected in respiratory tract
Natural Infection/ Mucosal Vaccination
Humans
Natural infection = longterm immunity
High titers of specific IgG and IgA in nasal secretions
Mice
Mucosal vaccination generates specific IgG and IgA in respiratory tract
---------------------------------------------------
Authors personal contestations to the development of mucosal vaccinations:
The admittance and pursuing of an alternative to systemic vaccinations is a huge step forward for the movement of vaccine awareness! I am certainly not one to shy away from that. However, the OPV (Oral Polio Vaccine), a mucosal vaccination, has been banned in the western hemisphere and many other parts of the world because it causes provocation poliomyelitis (has in fact caused a large number of cases of Paralytic Polio in India and Africa where it is still being used... because it's too dangerous for us but not for the pharma companies to sell or give away to starving children in developing countries). There are also the flu mist vaccines which go through the nasal mucosal portals, yet carry a risk of neurological disease and alzheimers (among other things), a much greater risk than the risk of the flu itself. So as far as the safety factor is concerned, mucosal vaccines may not be much of an improvement, if any. In terms of effectiveness, however, I remain optimistic and open minded about what mucosal vaccinations may potentially accomplish.
An additional thought is that the concept of stopping children from getting mild and innocuous childhood illnesses that build the immune system in place of supporting nutrition and Vitamin D supplementation is not something I like to support. The theory that perfectly healthy children need drugs and chemicals in their bodies is absolute nonsense, especially when the concept of "they must risking getting such and such frightening diseases so they won't get this other frightening disease" comes into play.
It's a fantastic thing that we are learning more about the complexities of the human immune systems and the role they play in our health; but let's not use it as an excuse to encourage our patients to leave parental responsibility (nutrition, exercise, etc) on the byway because we want to take the lazy road and just inject them with something instead. As any physician knows there is no "automatic" attainment of good health and a strong immune system, the maintaining and developing of such is something that must become a part of our daily lives and rituals.
Subscribe to:
Posts (Atom)